|
Last week both DRX and LH lowered 2018 guidance citing everything from the weather to softer genetic test volume. On Friday, the Government Accountability Office had more bad news. Its report, Medicare Laboratory Tests: Implementation of New Rates May Lead to Billions in Excess Payments, recommended further revisions to PAMA pricing methodology and called for an end (again!) of code stacking for panel tests. If each of these recommendations were implemented by CMS, Medicare would save $733 million and $10.1 billion, respectively, over three years. CMS has already begun implementing an anti-code-stacking policy and appears prepared to adopt changes to the reimbursement calculation. The report also recommended that CMS require all labs to report data and not just the 2,000 or so that meet CMS’s criteria under its interpretation of PAMA. CMS took steps to adopt this recommendation in the CY 2018 Physicians Fee Schedule Final Rule. |
The Government Accountability Office anticipates the Medicare payments in 2018 will be about 3 percent or $225 million more than in 2016, assuming utilization remains at similar levels.
Not exactly what Congress intended.
The CBO score at the time estimated a reduction in Medicare payments of $400 million in 2018 and $2.5 billion over ten years.

In response to the increase in Medicare lab payments, the GAO reviewed the implementation of PAMA and made the following recommendations:
- Collect complete private-payer data from all laboratories required to report or address the estimated effects of incomplete data
- Phase-in payment rate reduction that start from the actual payment rates rather than the maximum payment rate
- Use bundled rates for panel tests
Normally, we do what everyone else does when the GAO issues a report. We yawn. However, the speed with which CMS has responded to their criticism of late and the way in which Administrator Verma has lauded the Agency's record of reducing outstanding recommendations has required us to be more attentive to the GAO's work.
Data Collection. The first recommendation will be the only welcome news for the industry. They have complained since implementation about the exclusion of hospital laboratories and physicians practices. To reduce the regulatory burden, CMS had established a definition of the “applicable laboratory” required to report private payer reimbursement data that excluded the vast majority of labs in the U.S.
The labs that actually reported data as required by PAMA were a fraction of the 250,000 laboratories in the U.S. and were largely independent labs like LH and DGX
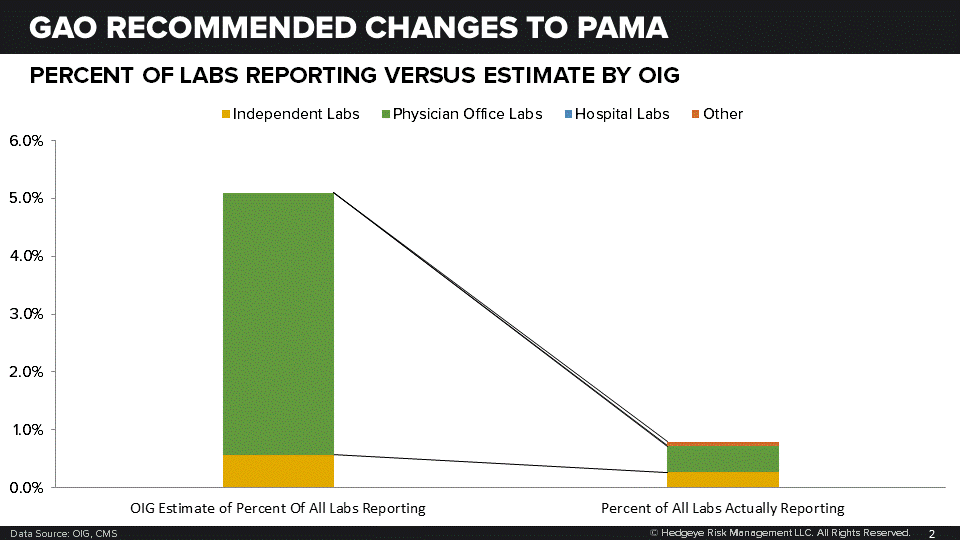
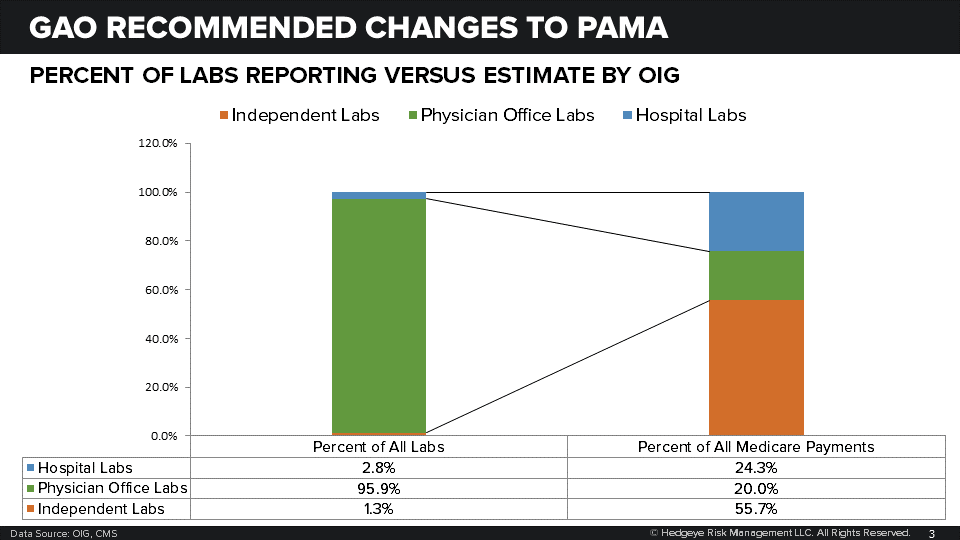
As both DGX and LH have pointed out, CMS’s approach meant that the private payer rates were, in effect, the rates paid to large independent labs like LH and DGX whose private payer reimbursement is generally lower than that paid to hospital and physician labs.
In the final CY 2019 Physicians Fee Schedule payment update, CMS began complying with the GAO’s recommendation by requiring more hospitals to report data.
Pricing Methodology. The second recommendation will not be welcome news to the industry. When CMS implemented PAMA at the beginning of 2018 they decided to apply the price increases and decreases dictated by the new private payer methodology to the 2017 National Limit Amount. They did this even though many tests were reimbursed not at the NLA but at a lower amount established by either actual payment history or the prices set locally by Medicare Administrative Contractors.
As we pointed out in our analysis of the final rule, CMS’s decision to apply the PAMA price reduction to the NLA and not the price Medicare was actually paying for the test, increased reimbursement for some tests. CMS’s methodology also resulted in reimbursement reductions being less than would be the case if the PAMA methodology were applied to the effective rate instead of the NLA.
For example, HCPCS Code 83036, Glycosylated Hemoglobin Test, had an NLA of $13.32 in 2017. The weighted median of private payer reimbursement was $8.50, a difference of ($4.82.) PAMA requires that the reimbursement not be reduced by more than 10 percent in 2018, so the final rate was $11.99. However, if the 10 percent downside limit had applied to the effective rate, which based on 2016 data, would have been about $13.17, the 2018 reimbursement would have been $11.85. In 2016, Medicare paid for about 14 million hemoglobin tests and would have saved about $2 million had it adopted the GAO’s methodology.
Similarly, MYGN’s Hereditary Cancer Test, HCPCS Code 81162 had a 2017 NLA of $2,503.26. The weighted median of private payer reimbursement was $1,615.81, a difference of $887.45. With the application of the 10 percent downside to the 2017 NLA, the 2018 rate was set at $2,252.93. If the 10 percent downside limit had been applied to the effective rate of $2,485.24, the 2018 rate would have been $2,236.72.
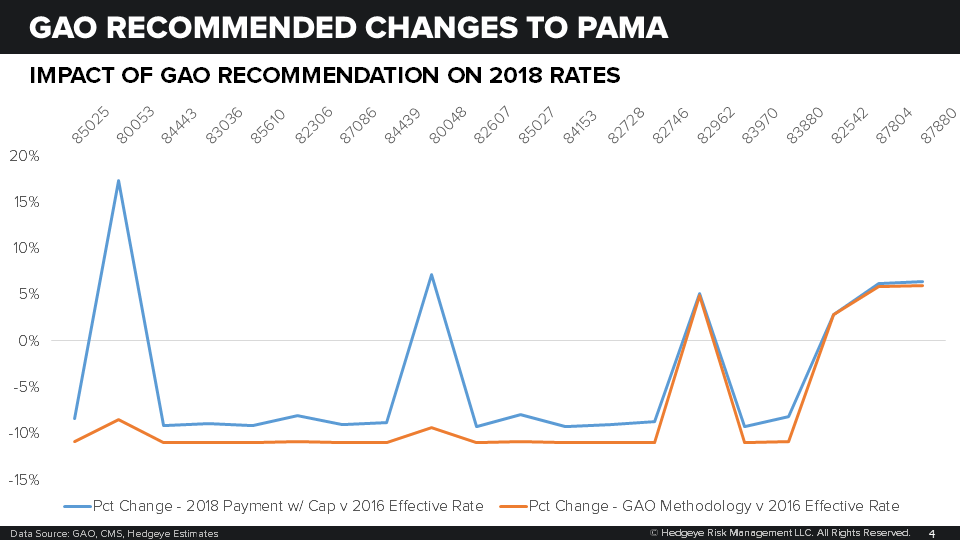
Had CMS applied the GAO’s preferred methodology in 2018, rates on the top 20 tests would have been reduced by more than 10 percent and certain rate increases would have been eliminated.
The incremental impact is a lot lumpier due to the variable differences between weighted median calculations and the 2017 NLA:
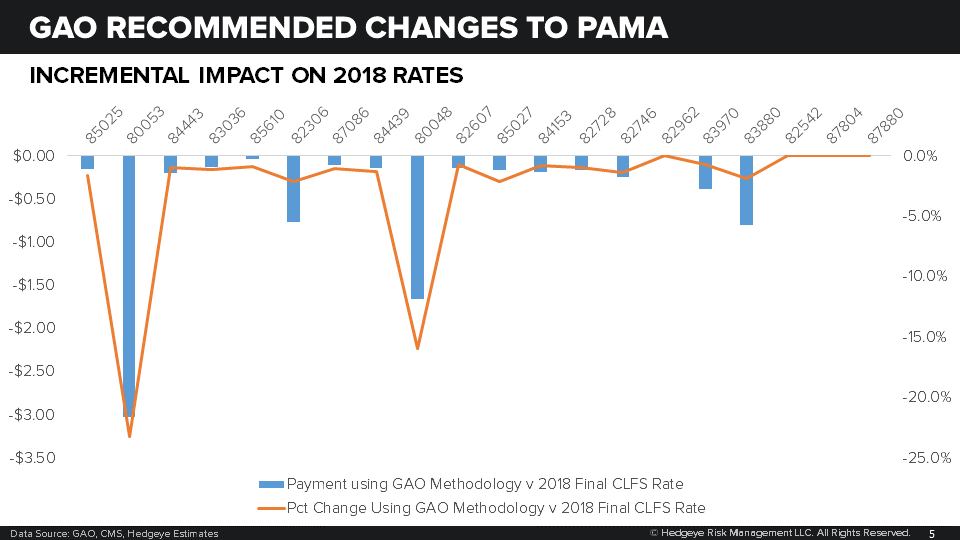
If CMS adopts the GAO’s recommendation, and they were non-committal in the report saying only that it would require additional rulemaking, then CMS will save about $120 million on the top 20 tests by volume. The GAO estimates that Medicare will pay $775 million more on all tests than would otherwise be the case had CMS applied the rate reduction to the actual rate instead of the 2017 NLA.
To recover the estimated $775 million, CMS could apply payment adjustments for CY 2019 and CY 2020 or reduce the payments for the next rate period of CY 2021 through CY 2023.
Bundled Payments for Panel Tests. The GAO’s last recommendation is that CMS reinstate bundled payments for panel tests for which there is no billing code. CMS had abandoned the use of bundled payments for panel tests without codes because it was concerned it would not be able to collect valid data on private payer rates.
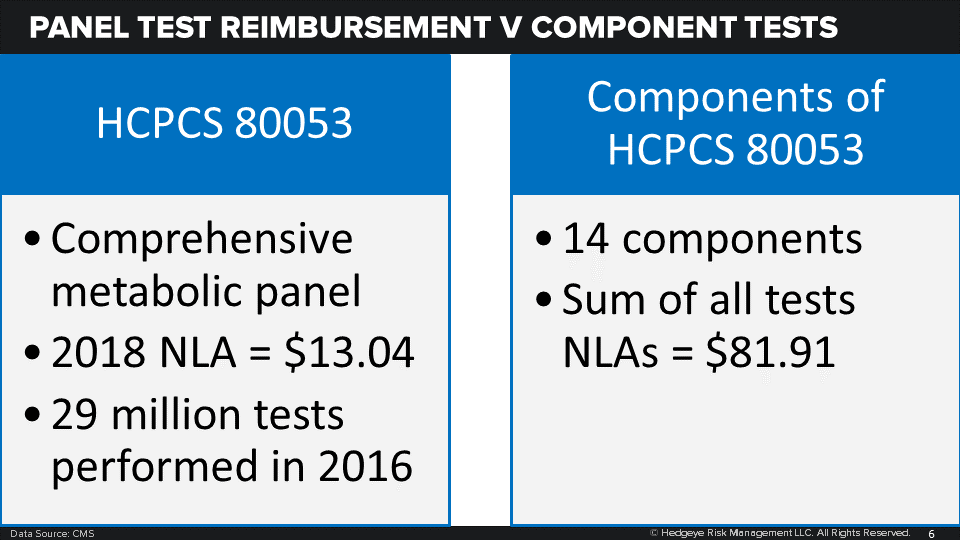
Similarly, laboratories that submit claims for any one of the panel tests that have a billing code can bill for each of the component tests within the panel. Prior to 2018, if a lab submitted a claim for a panel test with each component test billed individually, the Medicare Administrative Contractors would pay the bundled payment rate instead.
The GAO estimates that unbundling of panel tests with and without a code will cost the Medicare Trust Fund $218 million and $10.1 billion, respectively, over the period 2018 through 2020.
Fixing this problem will not be easy. It is a result of retrospective data collection and the variable way in which commercial payers reimburse for panel tests. In 2016, the CLFS Advisory Panel developed three options:
- Unbundle panels and pay for individual tests
- Use PAMA data for panels with codes; establish prices for panels without codes that limit number of tests for which there is reimbursement
- Create a G-code for individual tests and pay for CPT panel codes using PAMA data
The Advisory Panel adopted the first option which has given rise to the GAO’s criticism.
However, effective January 2019, labs will no longer be able to submit claims for components of a panel test for which there is a billing code. Two of the top 10 lab tests by volume, and LH and DRX’s bread and butter, are panel tests; HCPCS Code 80053, Comprehensive metabolic panel and HCPCS Code 80048 Metabolic panel. These tests had an estimate 2016 volume of 29 million and 4.6 million tests, respectively.
For tests for which there is no code, a fix will most likely be available for the next rate setting period since CMS could instruct labs to collect data on how commercial payers bundled panel tests – something they were not able to do in 2017. Worth noting is the policy change has the support of Congress which included instructions in the FY2019 appropriations to revise the way in which CMS pays for panel tests.
This change does not bode well for MYGN's MyRisk (R) panel. The MyRisk (R) panel test does not have its own code and is submitted as a stack of general MoPath codes. The impact on that test will depend on how CMS decides to address these code-less panels.

Call with questions.
Emily Evans
Managing Director – Health Policy
\
Twitter
LinkedIn
