
We suspect it is weeks like this one that made Donald Trump run for president. Perhaps understanding the consequences if the American Health Care Act were to fail, Trump was in full deal-making mode late last week and over the weekend. House conservatives were summoned to the White House. Conservative Senators Ted Cruz and Mike Lee met with White House staff at Mar-a-Largo and presidential adviser Steve Bannon was reportedly reaching out to members of the Freedom Caucus to involve them in negotiations to get the AHCA across the finish line.
A lot of the concerns about the bill are not easily fixed due to reconciliation rules. Governors, for example, want the bill to include some increased flexibility for states to manage their programs over and above that promised in two letters from HHS Secretary Tom Price last week. Conservatives want a work requirement for able-bodied Medicaid beneficiaries.
That is where Trump comes in. He and the White House team have declared the ACHC just one part of a three pronged effort to overhaul America’s health care system as a way to assure members of Congress on both the right and left. One-on-one negotiating sessions have included promises that the ACHA will be the first, not the last word from Trump on health care.
The effort is paying off. House leadership scheduled the vote for Thursday, a reflection of their confidence in the count.
Early next week, the House Rules Committee will post the version of the bill on which there will be a vote. The changes we anticipate are:
- Moving the end to Medicaid expansion from 2020 to 2018 or 2019
- Increasing tax credits for purchase of insurance for people 55 to 64
- Adding a block grant option to the per capita system for states looking for more flexibility in their Medicaid programs
- Adding a work requirement to Medicaid for able-bodied adults
- Inclusion of some expression of Congress's intent that states should be given maximum flexibility to manage their Medicaid programs
- Elimination of 30 percent continuous coverage penalty
It remains to be seen what the Senate does but increases to the tax credits for older adults and giving states a lot of flexibility to manage their Medicaid enrollments as they wish will go a long way toward appeasing moderates. Conservatives like Ted Cruz and Mike Lee are certain to like the block grant, work requirement and shorter fuse for ending the Medicaid expansion. Moderates will like the increased tax credits for older enrollees in the individual market.
As a reminder, the bill will not be making any stops in Senate committees and will proceed directly to the floor for a vote once it arrives from the House.
As for what it means to you:
We remain of the view that, while most Governors will act responsibly toward their Medicaid populations and their provider communities, it is hard to reach any other conclusions than the most radical change in Medicaid in 50 years is:
- Bad for inpatient hospitals that benefit from the frequently unnecessary emergency room volumes and inpatient care that could all be delivered in alternative, less costly settings. The end of supplemental payments to hospitals, particularly nonprofit hospitals, could be significant. Hospital-based physicians practices would be similarly affected.
- Disenrollment of Medicaid populations will increase bad debt and charity care although not to pre-ACA levels due to changes in accounting rules.
- In the near term, the ACHA is bad for Medicaid managed care which will see disenrollment through more frequent eligibility determinations.
- In the intermediate and longer term, it is good for Medicaid Managed Care Organization who’s per capitated payment model aligns nicely with a federal per capita and block grant financing system. This natural association will be further assisted by the end of supplemental payments to providers which have stymied managed care growth in some states.
- Good for mental health and substance abuse providers that have been limited by Medicaid rules even though their patients represent a significant cost driver in most Medicaid programs.
- Good for low cost provider types like urgent care clinics, ambulatory surgery centers, home health, primary care physicians practices and the services and devices that support them.
- A mixed bag for SNFs who have suffered as a result of Medicaid policies and payment bonuses that encouraged home and community based care instead of in a nursing facility. The open questions are whether they will get relief from their state provider taxes under a new financing mechanism.
- Neutral for pharma as the rebate system and other policies related to Medicaid remain untouched at this point. Note that Governors have put on their wish list the ability to end the requirement that all Food and Drug Administration-approved drugs be included in their formularies.
Changes to the individual market will be more muted because that population has already been subject to significant increases in cost sharing which has limited utilization. The individual market also represents a much smaller number of people than Medicaid.
- All provider types will likely be affected by the elimination of the actuarial value of plans but since the requirement that each plan include essential health benefits remains, the impact will be muted
- Hospitals will be negatively impacted by an increase in bad debt although how much of one is a question due to the already high deductibles
- In the long term, we anticipate that populations whose health insurance coverage is supported by tax credits or high risk pools or state-based reinsurance will be rolled together with Medicaid managed care populations to create seamless coordination of care.
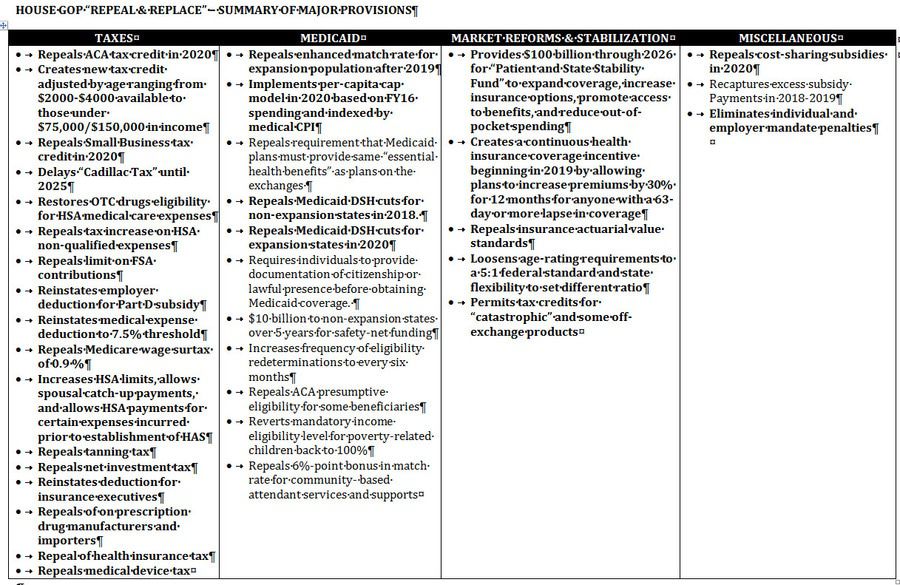
In case you lost it, here is your handy “clip and save” chart with the major provisions to the ACHA:
Call with questions. We are always here. If Congress’s octogenarians can stay up late, so can we.
Emily Evans
Managing Director
Health Policy
@HedgeyeEEvans
