
Below is a complimentary Demography Unplugged research note written by Hedgeye Demography analyst Neil Howe. Click here to learn more and subscribe.
Be sure to check out his highly anticipated new book, The Fourth Turning is Here, which is now available for purchase.
|
The FDA just approved Leqembi, a pricey new Alzheimer’s drug. It’s one of a growing number of drugs whose eye-popping price tags are sparking debate over whether Medicare and Medicaid should cover them. (NBC News) |
Earlier this month, the FDA granted full approval to the Alzheimer’s drug Leqembi. The approval means that the drug will now be covered by Medicare, expanding access to an estimated million people with early forms of the disease.
Leqembi, from Japanese drugmaker Eisai (ESALF) and U.S. partner Biogen (BIIB), has made headlines for being the first drug shown to slow the course of Alzheimer’s — and for its hefty price tag. The drug costs $26.5K annually before insurance coverage. Additional treatment, such as medical visits to receive the drug and regular brain scans, could drive the total to about $90K a year.
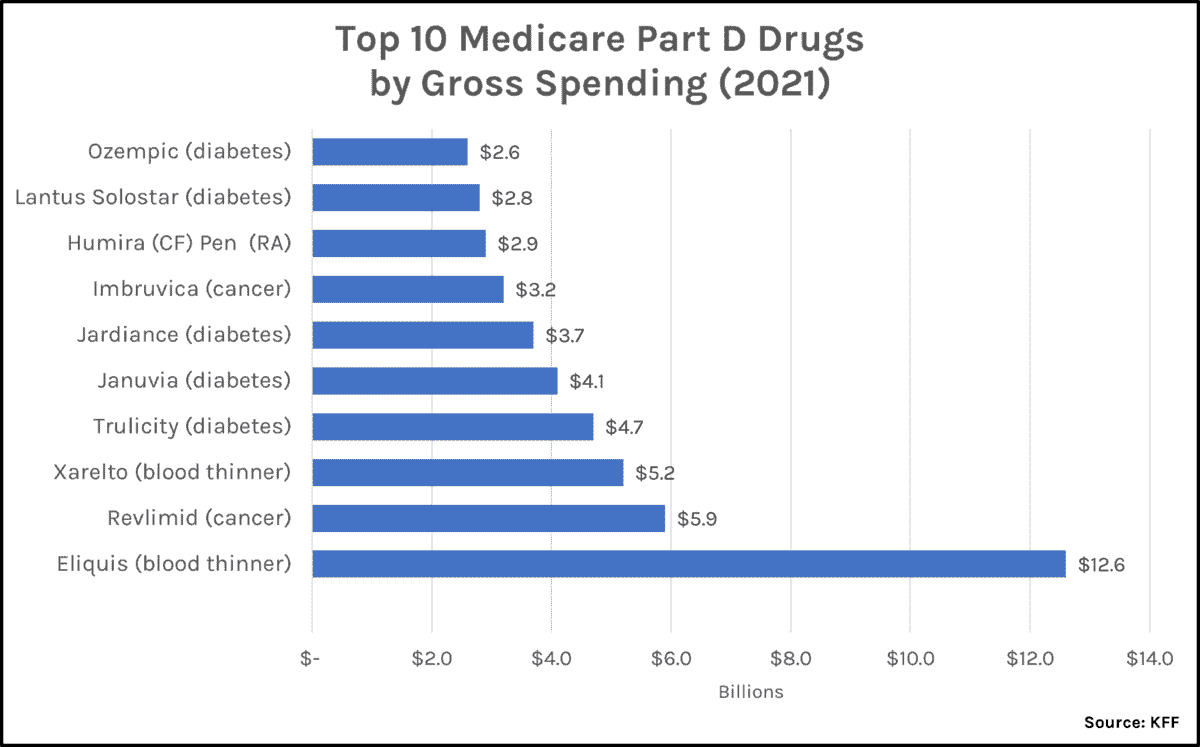
An analysis by KFF (formerly the Kaiser Family Foundation) projects that if just 10% of the 6.7M older Americans with Alzheimer’s takes Leqembi, it will increase Medicare spending by $17.8B. That would instantly thrust Leqembi into first place as Medicare's single costliest prescription drug. (The current frontrunner, as of 2021, is the blood thinner Eliquis, at $12.6B per year; see below.)
Yet many experts question why the FDA and Medicare are giving Leqembi the green light. Some say that the benefits that Leqembi provides to its target patients, those with early-stage Alzheimer's, are barely perceptible. Others doubt the amyloid hypothesis underlying both Leqembi and its predecessor Aduhelm (developed by the same two firms). Some even charge the hypothesis is based on fabricated data. What's more, even if Leqembi does generate some benefits to some patients, these may be cancelled out by side effects. An analysis from the Institute of Clinical and Economic Review concluded that, given the drug’s potential for brain bleeding and swelling, a fair price for its level of effectiveness would be no more that $8.9K, or two-thirds less than its actual price.
The questions surrounding Leqembi showcase a persistent dilemma facing the health care system. An increasing number of prescription drugs are hugely expensive. According to a recent JAMA study, the median price of a new drug was around $180K in 2021, up from $2.1K in 2008. These costly drugs are driving up the Medicare and Medicaid outlay burden on taxpayers and health insurance costs for employers. And without a method of limiting these costs anywhere in sight, American taxpayers, workers, and retirees are on the hook for an endlessly rising tab.
To appreciate the cost impact of new and super-expensive drugs, consider that Medicare Part D covers more than 3,500 prescription drugs. Yet of all these, the 10 costliest drugs comprise 22% of all Part D "gross" spending; the top 50 comprise nearly half of all spending. Spending on the top 10 has doubled from $22B to $47B in just the last three years, from CY 2018 to CY 2021.

According to the Peter G. Peterson Foundation, total U.S. spending on prescription drugs nearly tripled from $122B in 2000 to $348B in 2020. The Centers for Medicare and Medicaid Services project that this amount will rise further to $567B by 2030. (In case you're wondering, that's a 5.2% CAGR, well over a percentage point more than GDP growth.) Prescription drugs are one reason health care spending has consistently outpaced GDP growth over the past two decades, a gap that will widen as the share of older (and sicker) Americans grows. But we still don’t have any fair or rational way to evaluate the differential efficacy of pricey new prescription drugs.
Most of the time, it comes down to three basic problems:
First, the FDA and Medicare are often swayed by nothing more definitive than a Big Pharma trial demonstrating that a new drug has no disqualifying side effects and promises some significant benefit over the most common alternative treatment. But this standard is ridiculously inadequate. How "serious" can the side effect be before it is disqualifying? And how marginal can the benefit be and still be "significant"? If a firm is spending $100M+ on a population-wide efficacy trial, it is certain to throw up dozens of high t-ratio statistics casting the benefits of its drug in the best light possible. What about the benefits of competing treatment alternatives — which may be generic or unpatentable and in any case much less expensive? Alas, we can be sure that much less money and many fewer reliable numbers will be backing any arguments in their favor, regardless of their underlying efficacy.
To illustrate, take another look at the list of 10 top-selling Part D drugs. Two of them, Eliquis and Xarelto, are newfangled blood thinners. Are they really better, in all applications, than their now-generic predecessor, warfarin or their antediluvian forerunner, aspirin? Does anybody know? Or care? One major on-label use for both drugs is to prevent deep-vein thrombosis or embolisms after joint-replacement surgery. A recent study in the NEJM (n size = 3,424) concluded that, for this purpose, Xarelto could be replaced almost entirely (25 days out of 30 after surgery) by baby aspirin, at barely one penny per pill, with no difference in outcome.
Another five of the top 10 are drugs that treat Type 2 diabetes. One of the diabetes drugs, Ozempic, has exploded in popularity as a weight-loss medication (at a different dose) under the name Wegovy — whose maker, Novo Nordisk (NVO), recently spent more than $6M lobbying for Medicare to cover it. (Covering Wegovy and similar medications for every eligible beneficiary would almost double the entire Part D budget.)
But again, what about the alternatives? Studies show that an old generic standby, metformin, is just about as effective (and in some cases, more effective) in controlling the major indicators of Type 2 diabetes, including blood sugar levels, insulin sensitivity, and HbA1c. What's more, metformin is inexpensive, is well-known to be safe after decades of use, and indeed may extend lifespan (even in nondiabetics).
For some people, to be sure, the new-wave drugs are more effective at reducing BMI. But dietary and lifestyle changes alone may be an effective treatment for obesity—and these don't carry the risks of negative long-term side effects that are still unknown for the new injectables. Once again, opening up the taxpayer floodgate just because a new substance offers some benefit to some people is simply not an adequate standard.
Second, even after we establish that a drug is substantially more effective than any alternative, we aren't able to ensure that we are applying that effectiveness standard consistently across the health care system. How do we compare, for example, a new diabetes medication against a new treatment for hypertension or against another for malignant melanoma? Many other countries use metrics such money spent per quality-adjusted life years (QALY) gained. Starting with the assumption that they have a fixed budget, they use QALYs (or similar measures) to make sure they are maximizing the number of lives or the quality of life they can purchase with that budget.
If U.S. policymakers possessed such numbers, they could at least arrive at some rational standard for comparing alternative treatments. It goes without saying that our public budget for prescription drugs (whether in Medicare Part D, Part B, Medicaid, or the VA system) is finite. As we encounter endless new drug discoveries, we need some method of setting sensible priorities.
Finally, even if we are making consistent decisions across treatment options, there remains the final question: How much is too much? At the margin, how much is the public willing to pay for one more life saved? $100,000? $1,000,000? At what point do we say, no, we'd rather spending those resources on something else, like education or infrastructure or defense?
Consider the costliest drugs of all: gene therapies, which typically treat rare genetic diseases. Last year, the FDA approved the hemophilia-B drug Hemgenix, which at $3.5M for a single dose is the most expensive drug ever. But not by much. The hemophilia-A equivalent costs $2.9M; Sarepta Therapeutics’s (SRPT) treatment for Duchenne muscular dystrophy, $3.2M; Bluebird Bio’s (BLUE) treatment for cerebral adrenoleukodystrophy, $3.0M. And this list will only grow. The FDA has estimated that around 10 to 20 gene therapies will be approved each year through 2025.
In 2021, specialty drugs (including gene therapies) accounted for just 1.3% of Medicaid drug claims, but over half (53.8%) of the net drug costs. This share of spending has risen +115% since 2010. Hemophilia B affects 1 in 40K Americans. Cerebral adrenoleukodystrophy affects 1 in 21K boys. Reducing costs by scaling up really isn't an option in these cases. Ruth Lopert, a health economist at George Washington University, recently told The New York Times: “The situation simply isn’t sustainable. Countries simply aren’t going to be able to afford these products, at the prices that are being asked.”
When all the options are expensive, government agencies and private insurers still fight to save money, of course. But they do so with aggravating screening devices that infuriate everyone. Rather than move providers toward less costly treatment options, they try to ration availability by making patients jump through regulatory hoops to obtain access to these drugs. Often, patients can only “qualify” by getting seriously ill — as in, patients diagnosed with Hep C who needs to show liver damage before getting cured with Gilead (GILD)'s Sovaldi (originally, $84K per treatment, now only $24K). Or in patients who are obese and prediabetic and are told they must be fully diabetic before getting Ozempic.
President Biden's effort to reduce drug prices has resulted, notably, in a provision in the 2022 Inflation Reduction Act which requires the federal government to negotiate prices for certain drugs covered under Medicare Part B and Part D starting in 2026. If a firm refuses to engage in the "negotiation" process, it faces steep fines. But again, this approach doesn't address the fundamental problems at the heart of drug pricing. They won't be solved by giving the president a big club to beat down this or that drug manufacturer whenever a high price comes to public attention — an approach which several companies and trade groups are suing on the plausible grounds that it violates the Constitution's takings clause.
What we need instead is a willingness to take on the health care industry and change the entire process by deciding which new drugs are worth covering at all. When drugmakers spend billions on a new chemical or biologic and further millions on research studies showing that their products are worthwhile — with no counterweight on the other side in favor of less expensive alternatives or to speak up in favor of the taxpayer or of other public ends, we end up with runaway cost growth. We also end up with a system that is increasingly unaffordable for everyone.
|
To view and search all NewsWires, reports, videos, and podcasts, visit Demography World. For help making full use of our archives, see this short tutorial. |
* * *
ABOUT NEIL HOWE
Neil Howe is a renowned authority on generations and social change in America. An acclaimed bestselling author and speaker, he is the nation's leading thinker on today's generations—who they are, what motivates them, and how they will shape America's future.
A historian, economist, and demographer, Howe is also a recognized authority on global aging, long-term fiscal policy, and migration. He is a senior associate to the Center for Strategic and International Studies (CSIS) in Washington, D.C., where he helps direct the CSIS Global Aging Initiative.
Howe has written over a dozen books on generations, demographic change, and fiscal policy, many of them with William Strauss. Howe and Strauss' first book, Generations, is a history of America told as a sequence of generational biographies. Vice President Al Gore called it "the most stimulating book on American history that I have ever read" and sent a copy to every member of Congress. Newt Gingrich called it "an intellectual tour de force." Of their book, The Fourth Turning, The Boston Globe wrote, "If Howe and Strauss are right, they will take their place among the great American prophets." The follow-up book, The Fourth Turning Is Here, hit shelves this week.
Howe and Strauss originally coined the term "Millennial Generation" in 1991, and wrote the pioneering book on this generation, Millennials Rising. His work has been featured frequently in the media, including USA Today, CNN, the New York Times, and CBS' 60 Minutes.
Previously, with Peter G. Peterson, Howe co-authored On Borrowed Time, a pioneering call for budgetary reform and The Graying of the Great Powers with Richard Jackson.
Howe received his B.A. at U.C. Berkeley and later earned graduate degrees in economics and history from Yale University.
