
(Note: We will be diving into the DVA model some more via webcast on Wed. Nov. 2 @10am ET. Please join us. Link here.)

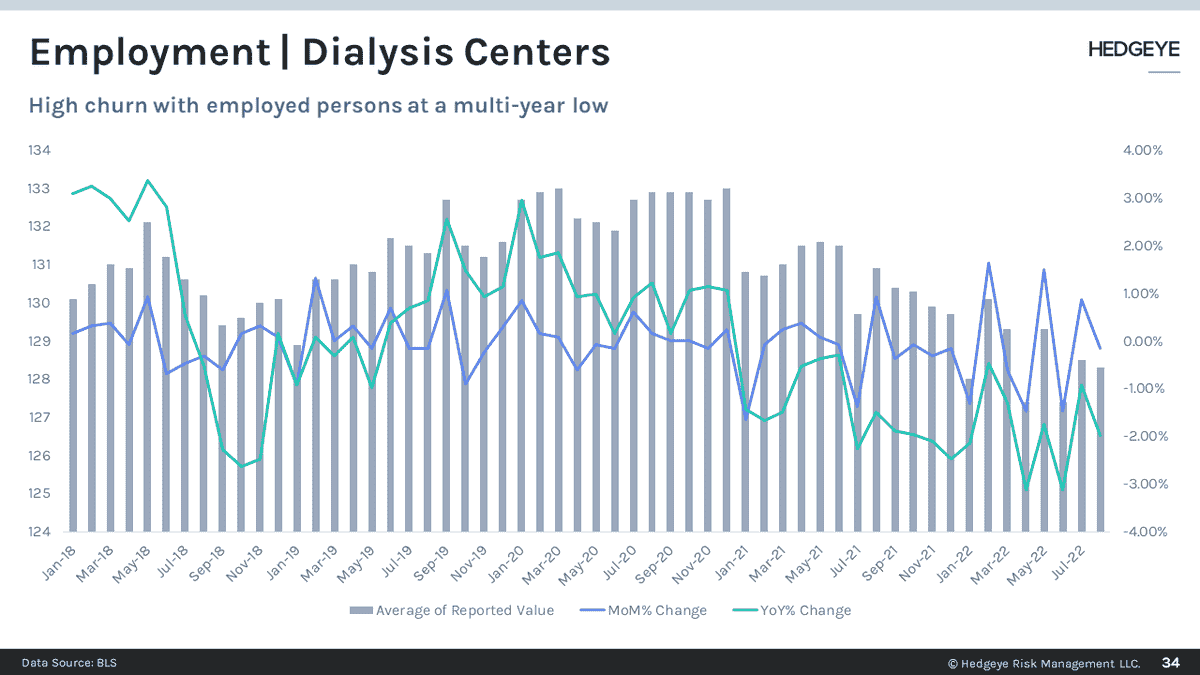
DVA CEO Javier Rodriquez seems baffled. The company slashed 2022 guidance by $200M and declared a virtually end to what Wall Street considered DVA's one redeeming feature, share repurchases. The culprits are high wage expense and lower volumes. In the case of the former, the problem is a simple one. Dialysis clinics compete with restaurants, retail and other low wage employers. Churn, a problem cited by Mr. Rodriquez, is clearly evident in the BLS' monthly employment report. The company is paying hiring and training costs only to see those workers depart for greener pastures.
The labor problem may get fixed by higher Medicare reimbursement as the elevated Employment Cost Index washes through in 2023 and 2024. Much will depend on demand in the competing non-health care sectors.
Lower volumes are another matter and thus far have mystified management. They admit to having low visibility into the Chronic Kidney Disease population which in and of itself is an indictment of their competency in managing a frail and vulnerable population. New admits are about 2,000 below normal. Under a baseline scenario, new admissions should run about 33-35k per quarter with DVA's share about 14-16k so a decline of 2k in a quarter is substantial.
Volumes are also affected by missed treatments. The company reports about 1/2 of missed treatments are a result of hospitalizations which addresses, in part, the third driver of lower volumes, excess mortality.
The company offers no explanation, only that they expect the "cumulative impact" of COVID to continue. Covid deaths nationwide have not disappeared but they are lower than they have been in all prior periods except 3Q 2021. Covid itself, then, is not an entirely satisfactory answer. We have offered in the past the possibility that, post-COVID, Americans are less healthy. That too seems like another partial explanation as it would also argue for higher new admissions, not lower.
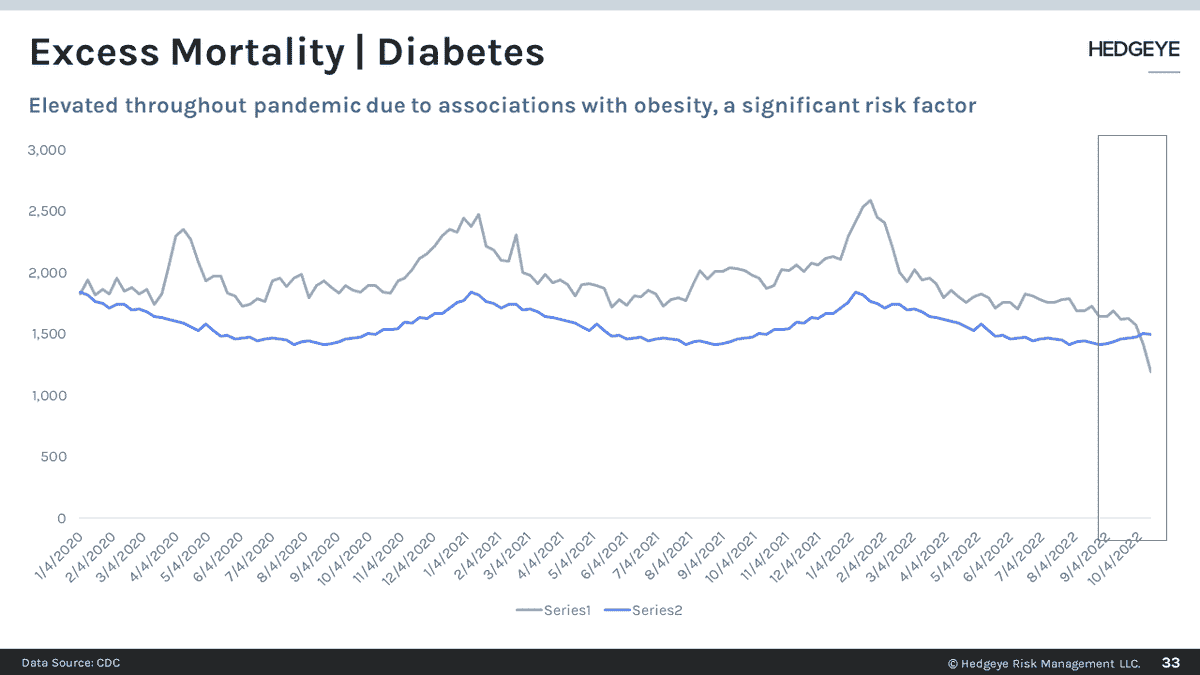
Perhaps, as the company has suggested, there is a "pull forward effect." Existing ESRD and CKD patients experienced higher mortality from Covid but have not been replaced yet by new patients. The excess mortality among diabetes patients may argue against that scenario. Throughout the pandemic, the deleterious effects of Covid on diabetics is clear and well known. Diabetes, often accompanied by obesity and hypertension, is the single biggest comorbidity associated with renal failure
The final possibility is that mRNA vaccines are having an adverse effect on this particular patient population. Unlike the diabetic population, death from kidney related disease, exhibits an unusual pattern, hugging the baseline until spring/summer 2021 then accelerating and remaining elevated since. Is it mere coincidence that excess mortality for people with renal disease accelerates with the mRNA vaccine roll-out? With no research to suggest one way or another, we leave it as an open question but one with a data signal clearly on the side of "no."
Please join us on Wednesday and we will dig deeper into the data.
Emily Evans
Managing Director – Health Policy
Twitter
LinkedIn
