
Top of the Funnel | Macro Data, Policy Position Monitor
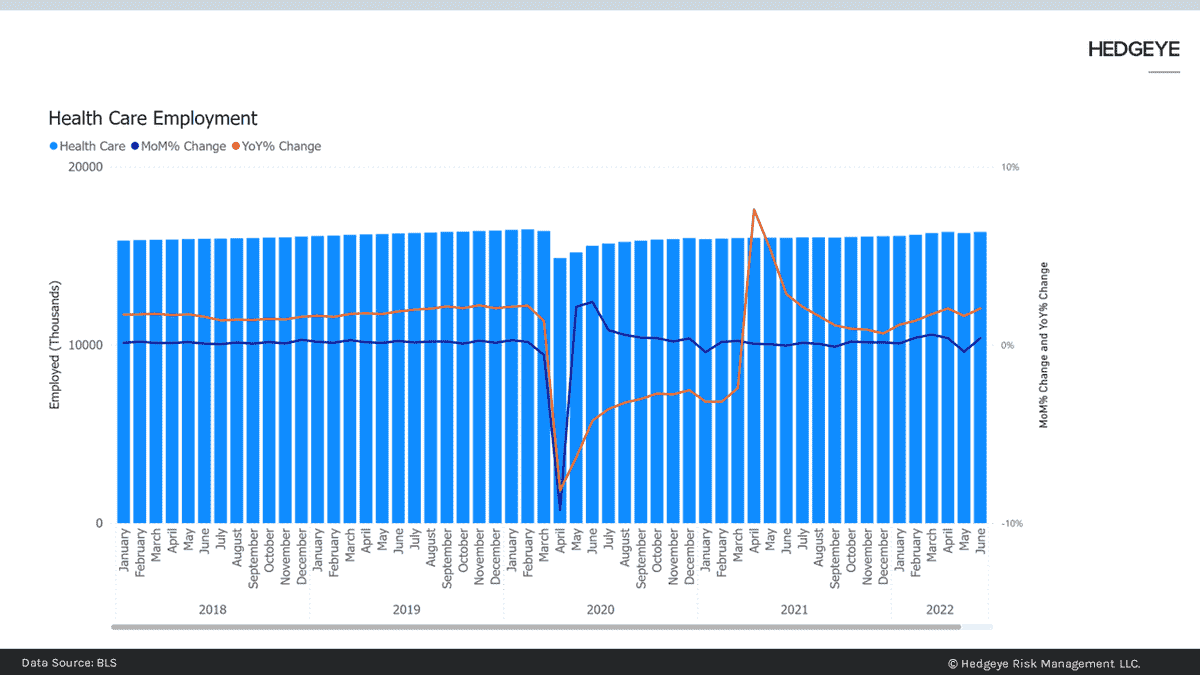
August Employment. HCA (+), THC (+), HUM (-), (ANTM (-) ENSG (+), NHC (+) DVA (-) Another sign health care will continue to earn its reputation as a shelter in the Quad 4 storm. Employment for all of health care continued its upward YoY trajectory in August, adding $16,405 jobs. Total employed in health care now exceeds the number of workers in March 2020.
Aggregate hours worked increased in July while average hourly earnings were essentially flat on a MoM basis. Meanwhile, women employed in Temporary Health Services – of which some part is nurse staffing – continues the rollover in July that began late in 4Q.
Employment in the supply chain also offers a rosy picture with overtime in July up 3.4% sequentially for Medical Equipment and Supplies Manufacturing.
Closely watched by us, because it is an exception, generally, to the robust growth in health care, is employment at dialysis clinics. It has been down and to the right since late 4Q 2020. On a MoM% basis, employment increased 71 bps but remains (1.08%) lower on a YoY% basis.
Also notable, left-for-dead nursing facility employment continues its slow acceleration from the post-COVID nadir in Sept. 2021
As a result of that rebound in nursing facility care employment, we have moved ENSG and NHC to the long side of the Policy Position Model, which you can find here.
September Employment Chartbook can be found here.
CONGRESS
Continuing Resolution. PFE (+), MRNA (+) BNTX (+) DGX (+) ABT (+) The White House submitted, as part of the expected Continuing Resolution to fund the government after the September 30, 2022- end of the fiscal year, a request for $22B in funding for pandemic response. That request includes $7B to purchase more vaccines, monoclonal anti-bodies and pre-exposure prophylaxis.
Recall that the administration has been rebuffed in previous requests even though they claimed they were running out of money. When they repurposed funds from other uses, they met with the ire of the normally very mild-mannered Sen. Mitt Romney.
Also consider the administration had expressed a goal transitioning the financing mechanisms for COVID-related services to the traditional sources, Medicare, Medicaid, and commercial insurance. The fist two are easily accomplished Commercial insurers, however, usually develop medical policies in conjunction with their coverage decisions. If that process is slow to develop, the White House may be feeling some pressure to keep the federal gravy train running.
The request also includes more money for testing even though official policy is to test symptomatic individuals, which would imply insurance coverage.
More of the usual muddled messaging and hard to know what Congress will say about the price tag. If they are convinced PFE and MRNA may have a glide path to reimbursement in 2023. If not, it looks more like a spending cliff.
VALID Act No More. ILMN (+), NVTA (+), NTRA (+), MYGN (+) Attached to a CR, should be a clean FDA User Fee bill. Time is running out to reach agreement on regulation of in vitro lab tests. The Senate sponsor, Richard Burr, is retiring and the FDA needs authorization to continue operations.
The VALID Act would have established a risk stratified approach which almost guaranteed genomic tests would be more heavily scrutinized than in the past. There is agreement on regulation but not enough to get it through in 2022. Might be a 2023 or 2024 project if someone picks up Sen. Burr’s baton.
THE WHITE HOUSE
Medicaid Enrollment. ANTM (+), MOH (+), CNC (+) CMS released new proposed guidance for states on Medicaid and CHIP eligibility. The new guidance offers changes that, in many cases, are long overdue such as eliminating the waiting period for new CHIP enrollees and standardizing eligibility and enrollment processes.
Other changes are probably designed to delay disenrollment – warranted and not. Redeterminations would be limited to once every 12 months and beneficiaries would have 30 days to respond to requests for information. The White House is concerned that, once the Public Health Emergency ends, the uninsured rate will rise quickly, giving the president a political problem ahead of the 2024 election.
Vaccines. PFE (+), MRNA (+), BNTX (+) The FDA and the CDC have now cleared PFE’s new bivalent COVID shot. The CDC guidance suggests that a person is “fully vaccinated” if they have the primary two dose course and the new bivalent dose. That means that someone who has taken the primary course and the two boosters would need a fifth shot to comply with the “fully vaccinated” requirement of employment or military service.
The CDC is also sending a muddled message on shot cadence. The Adcomm was clear that a bivalent shot less than 2 months after infection or a booster, was not advised. The CDC Director, Rochelle Walensky suggested that anytime was a good time to get the shot. CVS and WBA say they are ready to begin administering shots as early as next week.
Other Stuff
Medicare Payment Updates.(AME D (+), ENSG (+), NHC (+) Medicare released its latest reimbursement models. It is finally catching up to labor costs and inflation. Too late for 2023 payment year but should bode well for 2024. Link to IPPS spreadsheet here.
Recent Events
The Failure of (Federal) Science, A Discussion with Dr. Tracy Beth Hoeg
Searchable calendar of weekly events and notes can be found here.
Have a great long weekend.
Emily Evans
Managing Director – Health Policy
Twitter
LinkedIn
