
|
Editor's Note: This is a complimentary research note published by Healthcare Policy analyst Emily Evans. CLICK HERE to get daily COVID-19 analysis and alerts from our research team and access our related webcasts. |

In the crazy (and I would argue bad for your health) world that has political reporters covering a science and medicine issue, the focus has been on the facile (also bad for your health) like shut-down orders, wearing of facemasks and, most recently, "mass" testing for the presence of COVID-19.
The popular emphasis on these easily understood ways - with little scientific consensus - of measuring government response to the COVID-19 outbreak has left the public wondering when life will become more pleasant. Stubbornly high new confirmed cases seem to suggest "never."
In most cases, however, a decision to impose and relax certain restrictions on commerce and assembly is a complex one. Case volumes are a factor, of course, but they are viewed through the lens of other equally important considerations. These include:
- Inpatient Hospital Capacity – The chief public health consideration for ordering mandatory closure of businesses and religious gatherings is protection of the health care system and its workers. A health system already full of seasonal flu patients as COVID-19 cases appear in a community will accelerate imposition of restrictions where a half full hospital does not.
- ICU Capacity – Respiratory diseases like COVID-19 and other Influenza-Like Illnesses are successfully treated when there is available advanced care in the form of ICU beds staffed with properly trained pulmonologists, respiratory therapists and the necessary supplies and equipment, including PPE and ventilators.
- Positive Test Rates – High rates of positive tests in a community indicate the presence of disease among symptomatic and asymptomatic individuals that could put pressure on the health system if symptoms develop in too many people.
- Influenza-like and COVID-like Illness ER Treatment and Inpatient Admission – The decades-old measure of ILI admissions and ER counts has been augmented by surveillance for COVID-like – cases presenting with all of the symptoms of COVID-19 but without a laboratory confirmed test – and was effective in signaling the spread of COVID in Washington State and New York City in February.
- Hospitalization Rates – COVID-19’s disparate impacts depending on population attack mean the disease can present in a community differently, such as Nashville which experienced an attack of younger residents, with a low impact on hospitalizations. An attack on an older population will have a different result.
Each state is paying attention to these metrics but weighing them differently and always cognizant of the optics associated with relaxing standards when caseloads are increasing. The Governor of Mississippi recently walked back changes to his stay-at-home order due to sharp increases in confirmed case volumes. Meanwhile the Governor of Nevada got creative and has decided to redefine COVID-19 caseloads to mean:
Consistent and sustainable downward trajectory of COVID-19 cases and decrease in the trend of COVID-19 hospitalizations over a 14-day period. This will be measured by:
- Decline in percentage of people testing positive.
- Decrease in the trend of COVID-19 hospitalizations.
This new definition craftily allows the Governor of Nevada to avoid that whole confirmed case count thing that has driven the news cycles so much recently.
There are 50 different approaches to relaxing stay-at-home orders but they do boil down to the few aforementioned important data points that can be weighed against the political environment and the experience of each state.
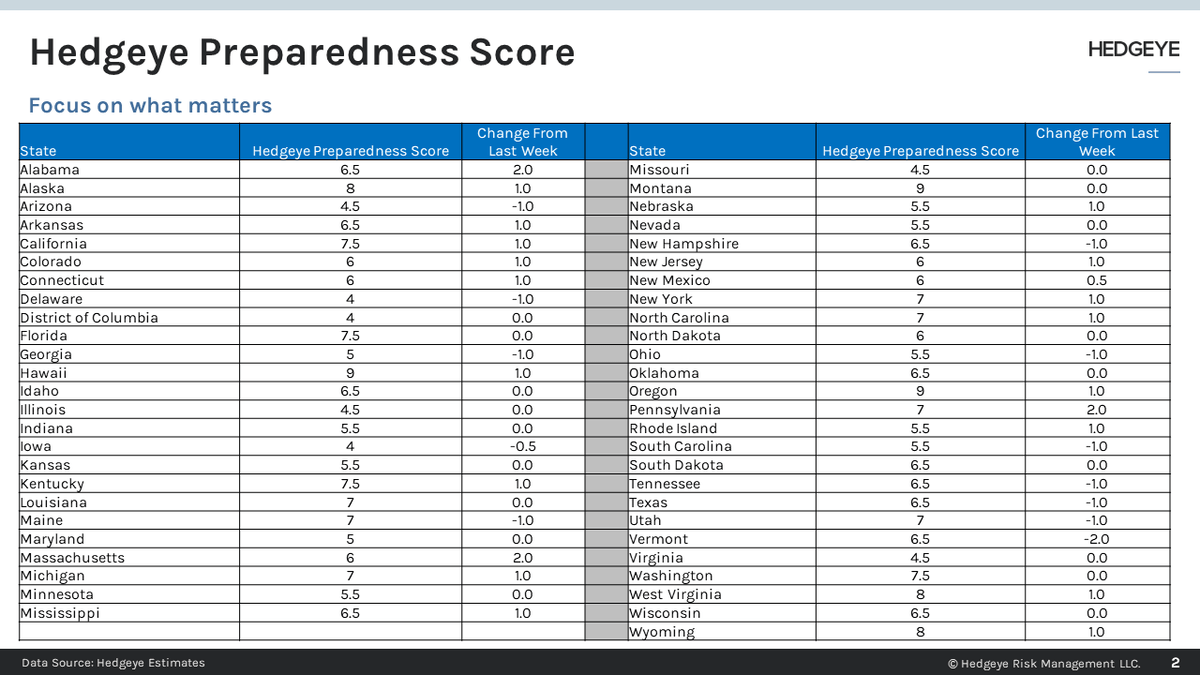
To make it as easy as possible for our clients to get a quick handle on where progress is being made, we developed a Preparedness Score. The Hedgeye Preparedness Score weighs 14-day increases and decreases in confirmed COVID-19 cases, positive test rates (assuming flat or increasing test volumes) and ILI ER Visits on an 9-point scale. Beginning next week, we will be adding new data available on hospital inpatient and ICU capacity, that is now collected by the CDC, at which point the scale will be filled out to 10 points.

The CDC is currently providing data on COVID-19 hospitalizations in select states. Due to the limited availability, we will not be including it in the Preparedness Score at this time but will consider it in the broader political context in which Governors find themselves.
Quantifying a state’s progress helps remove a lot of the anecdotal noise and focuses on much of what Governors themselves are concerned with, not just for reopening but for the ongoing protection of their populations.
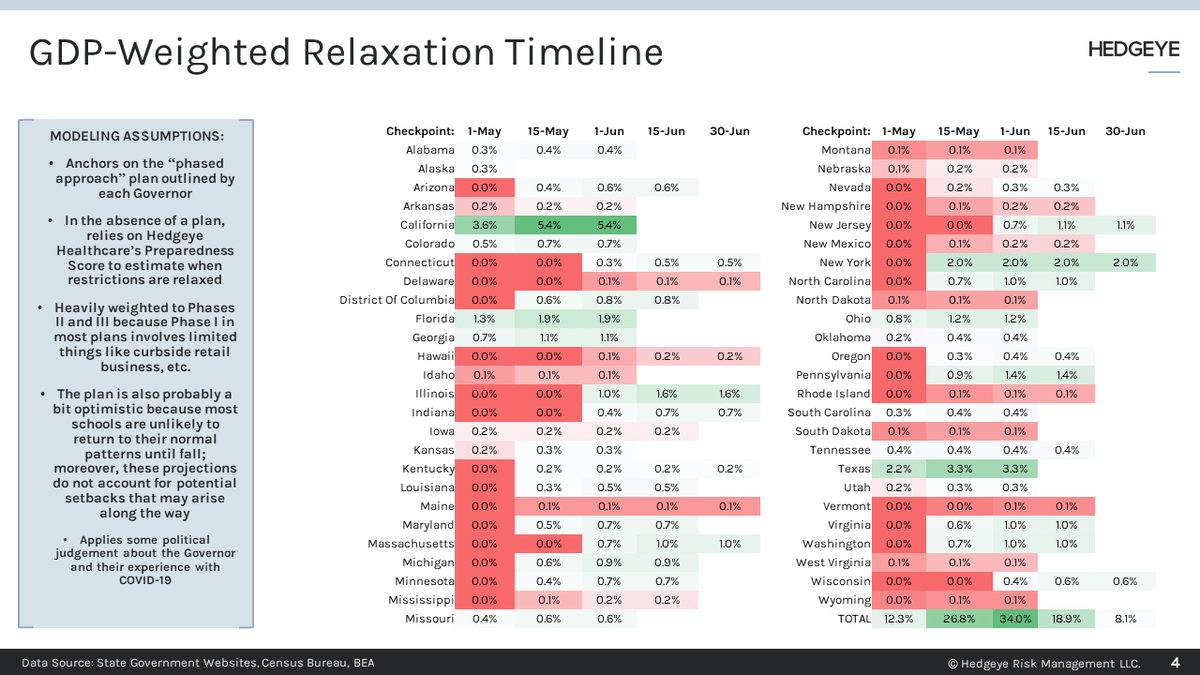
The Hedgeye Preparedness Score also allows us to build population and GDP models (h/t Darius Dale from the Macro team) that illustrate the impact of Governors’ changing policies. To build these models we sprinkle on top of our preparedness analysis a bit of politics.
The politics of Texas will and have spurred (no pun intended) Governor Abbott to quicker action than a pace tolerated in California. The State of Tennessee is getting credit for relaxing standards, except all its major cities (read: GDP) are still under some stay-at-home order as Gov. Lee defers to blue mayors in his red state.

Notwithstanding the fact that today is Tuesday, we will endeavor to get you updated Preparedness Scores and models each Monday. Nashville, where I live, apparently offended the karmic balance of the universe because Sunday night we enjoyed a dechero storm to go with our plague, our tornado and an executive order to halt live music.
We hope things improve soon so we can stay on schedule.
