
Pending at CMS are nine Medicare Payment rules and one general regulatory burden reduction rule. Under normal circumstances, these rules would be pretty routine affairs. As we like to point out every chance we get, these are not normal circumstances.
The Trump administration has taken a very different view of Medicare payment policy than the Obama administration (and, for that matter, the Bush II administration). Gone is the emphasis on “value-based purchasing” and other programs like Accountable Care Organizations designed to limit utilization. Instead, the Trump administration seems much more interested in policies that would reduce prices by encouraging competition through increased market entry.
This year is the first in which the Trump administration has complete control of the administrative policy machinery and they will no doubt use the levers to shape payment and delivery systems in accordance with their philosophy.
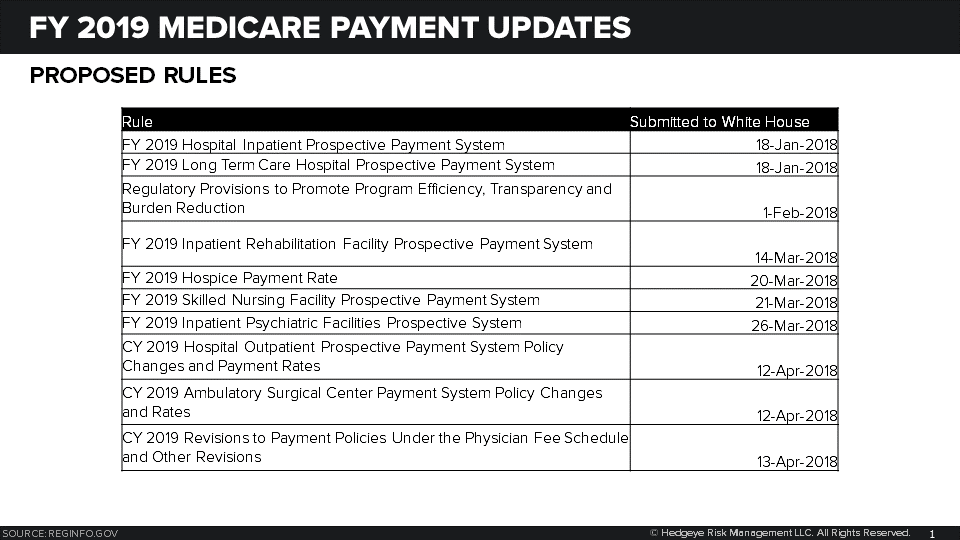
Likely to emerge first is the FY 2019 Hospital Inpatient and Long Term Care Hospital Prospective Payment System which cleared the White House Friday afternoon.
FY 2019 Hospital Inpatient Prospective Payment System.
The estimated Medicare payment update for FY 2019, based on current marketbasket forecasts, is:

There hasn’t been much innovative policymaking on the hospital front as CMS has instead sought ways diminish inpatient hospitals’ role as the dominant site of service by adjusting policy for alternative providers like Ambulatory Surgery Centers and Hospital Outpatient Departments. However, there are a few policy initiatives to keep an eye on.
DSH Payments. In August 2017, CMS began phasing-in a new method of accounting for uncompensated care for the purposes of distributing Medicare DSH payments to hospitals. Instead of relying on proxies of Medicaid days and Medicare SSI days, CMS began using uncompensated care reported on a hospital’s cost reports.
In 2018, CMS used a blended approach by incorporating cost report data for one year. In FY 2019, two years of cost report data will be used. By FY 2020, use of proxies will be eliminated.
Why you care:
The use of Medicare SSI and Medicaid days favors nonprofit hospitals located in states which expanded Medicaid. A shift to using actual data for uncompensated care will level the playing field so nonprofit hospitals in non-expansion states should benefit.
The use of cost report data on uncompensated care will also mean fewer Medicare dollars will be used to support uncompensated care at hospitals that treat a high number of Medicaid patients.
Effective with the ACA, hospitals do not receive 100 percent of the DSH pool of money as they did before passage of the law. Part goes toward uncompensated care payments and part is returned to Medicare Part A trust fund as savings, assuming the rate of uninsured remains below the 2013 level.
For FY 2018, CMS estimated that $16 billion would be distributed via DSH payments allocated as:
- 25 percent the pool distributed on the traditional DSH formula
- 75 percent divided as follows:
- For every 1 percent decline in the rate of un-insurance, the share of the remaining pool allocated to trust fund savings increases by 1 percentage point. CMS estimated that the rate of un-insurance had declined 42 percent since the passage of the ACA so 42 percent of the $12 billion, or $5 billion, of the DSH pool will be savings for the Medicare trust fund
- The remaining $7 billion ($12 billion * 58 percent) was distributed to pay for uncompensated care at hospitals.
Why you care:
The Office of the Actuary estimates that the percentage of insured people will decline in slightly in 2019 and beyond. The result will be more money for DHS eligible hospitals.

Social risk-factors. In last year’s rulemaking, CMS asked for comment on when and how social determinants of health could be incorporated into payment adjustments made via value-based purchasing and quality reporting programs.
The Assistant Secretary for Planning and Evaluation has conducted a number of studies and came to the very unsurprising conclusions that:
- Medicare beneficiaries with social risk factors (i.e., dual eligibility, residence in low-income areas, Black race, Hispanic ethnicity, rural residence, disability) had worse outcomes on quality measures
- Providers that disproportionately served Medicare beneficiaries with social risk factors tended to have worse performance on quality measures, even after accounting for beneficiary mix
ASPE has also suggested three possible policy responses:
- Adjust quality and resource use measures
- Stratify providers into groups by proportion at-risk
- Create separate payment adjustments
MedPAC favors the second of those three options.
Why you care:
As patient mix shifts to Medicare, every dollar counts. Hospitals in rural areas – like those owned by LPNT and CYH – will benefit from any payment adjustments that recognize the populations they treat.
Changes to MS-DRG subject to post acute transfer. The Bipartisan Budget Act of 2018 added hospice discharges to the post-acute transfer policy. Under the post-acute transfer policy, hospitals are paid less for patients discharged early to other sites of care except hospice.
The addition of hospice to the post-acute transfer policy is effective for discharges after Sept. 30, 2018, and as such will be a topic for rulemaking this cycle.
Why you care:
About a third of the 300,000 hospital discharges to hospice would be subject to the transfer policy. The CBO estimates the government will save about $500 million in FY 2019.
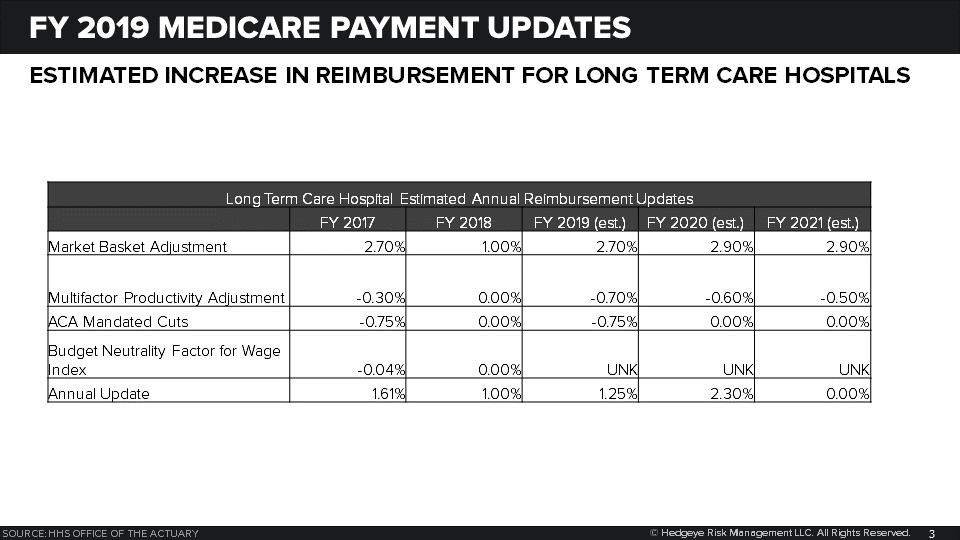
FY 2019 Long Term Care Hospital Prospective Payment
The estimated Medicare payment update for FY 2019, based on current marketbasket forecasts, is:
What to watch for:
The Bipartisan Budget Act of 2018 extended the current formula for site neutral payments through the end of FY 2019. To partially offset the cost, Congress imposed a 4.6 percent haircut on-site neutral payments made for FY 2018 through FY 2026. The payment update will include information on how the 4.6 percent payment reduction will be assessed.
The 25 percent rule that limits the number of patients a hospital can admit from a single acute care hospital was set to go into effect in FY 2017. However, CMS imposed a one year moratorium in anticipation of additional legislation. Such legislation has not happened and it would appear the CMS would need to implement the rule.
The real action policy-wise is going to be in the outpatient areas as the Trump administration wants to move as many services as possible to lower sites of care. Those rules should be out in a few weeks.
Call with questions.
Emily Evans
Managing Director
Health Policy
