
|
OVERVIEW: CMS is asking for feedback on potential changes to the Medicare Part D program that are designed to address at least one cause of drug price inflation: the web of rebates and concessions between plan sponsors, pharmacy benefit managers and pharmacy networks and drug manufacturers. This new policy direction would lower beneficiary cost-sharing at the point of sale making the idea popular with senior citizens if not PBM lobbyists. Specifically, CMS is suggesting, but not yet actually proposing, that it consider two significant policy changes:
These policy ruminations fall squarely into the Trump administration’s view that, to the extent drug manufacturers discount their prices, Medicare enrollees should benefit. Changes to the 340B drug discount purchasing program are another example of that policy priority. In 2015, about $25 billion was diverted from drug manufacturers to Part D plan sponsors and their PBMs in the form of rebates and concessions. If even a portion of this amount was passed through to Part D enrollees, the impact could be meaningful to CVS, UNH and HUM. Depending on how the policy is implemented the impact could also be felt by high price-high rebate brand name drugs. |
BACKGROUND. In January, CMS began signaling its dissatisfaction with Part D plans when it published, for the first time as far as we can tell, a news release titled Medicare Part D – Direct and Indirect Remuneration (DIR). In that report, CMS took note of the widening gap between gross and net drug costs and identified three important trends influenced by the growth of DIR:
- Cost-sharing – Beneficiary coinsurance payments are calculated based on the negotiated price at the point of sale so enrollees do not benefit from post-sale rebates, concessions and discounts paid by drug manufacturers or pharmacies.


- Subsidy Payments – Medicare pays Part D cost-sharing obligations on behalf of about $12 million low-income Medicare beneficiaries. As rebates and other price concessions shift the cost burden to beneficiaries, Medicare’s payments to low-income enrollees also increase.

- Plan Liability – High priced drugs, which are closely associated with high rebates, have shifted more of Part D spending into the catastrophic phase where plans are only responsible for 15 percent of plan costs.


In describing these trends, CMS also acknowledged that rebates had the effect of keeping Part D plan premiums low.

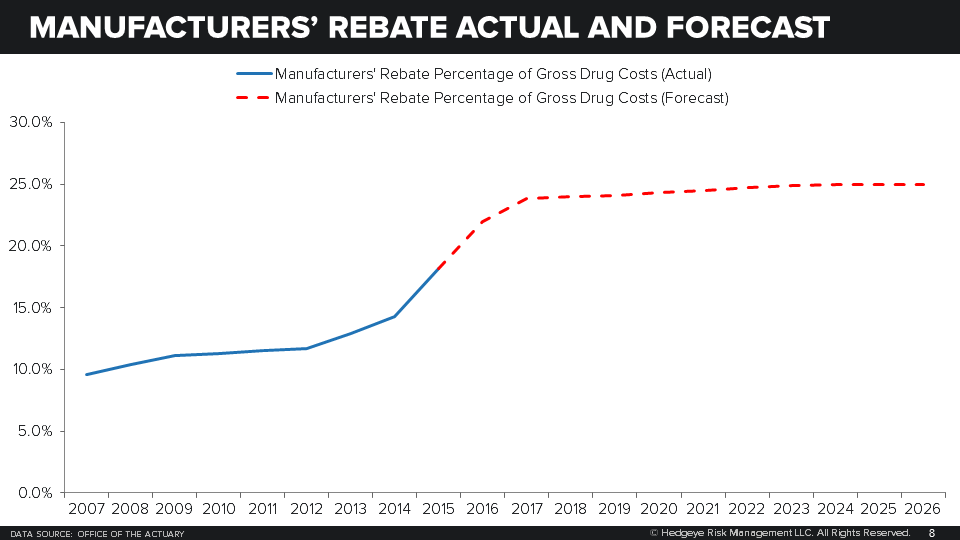
CMS is prohibited from disclosing manufacturer rebates and other concessions. The Office of the Actuary does, however, report aggregate numbers on “manufacturers’ rebates.” CMS reports more granular data on a rather significant lag – the most recent numbers are from 2014.
What data we do have suggest that manufacturers’ rebates, which account for the majority of DIR, have in recent years exceeded the spread between payments made by the federal treasury, premiums paid by enrollees and cost-sharing at the point of sale.

The growth in rebates has accelerated in recent years although the Office of the Actuary expects growth to stabilize in 2018 at about 25 percent of gross drug costs.
Separately, CMS indicated that they have noticed that a growing proportion of Part D sponsors and their PBMs have entered into payment arrangements with network pharmacies in which reimbursement is adjusted after the point of sale based on the pharmacy's performance on various measures defined by the plan sponsor or PBM.
According to annual DIR data submitted to CMS but not shared with the public, plan sponsors have been recouping increasing sums from network pharmacies after the point of sale for poor performance. These sums are far greater than those paid to network pharmacies after the point of sale for high performance. The most dramatic increases have taken place since 2012, according to CMS.
POLICY CHANGES. CMS is suggesting that it should require Part D plans to share the rebate largess with their customers. Specifically, CMS would like feedback on requiring a certain specified minimum percentage of the cost-weighted average of rebates provided by manufacturers in the same therapeutic category or class be passed on the Part D plan enrollees at the point of sale. Any amount in excess of the rebates passed on to beneficiaries would be treated as DIR at the end of the coverage year.
CMS does not name a percentage but says it would consider setting the rate below 100 percent. In the rule they provide results of their modeling which considered percentages of 33, 66, 90 and 100 percent. The balance, CMS indicates it is trying to strike, is between cost savings for beneficiaries at the point of sale and Part D plan premium increases.
To arrive at the average rebate amount that would be applied at the point of sale, CMS is suggesting a few policies on which it invited comment:
- Rebate amounts would be based on average anticipated manufacturer rebates for each drug category or class for the current year rather than using historical rebate experience.
- Only drugs for which a manufacturer provides rebates would be included in the calculation
- Average rebate amounts would be calculated separately for each plan
- Rebate percentages would be weighted so high price-high rebate drugs would be more influential on the passed through percentage
To address the growth in post point of sale incentive payments, CMS is also suggesting that it would like to consider changes to how Part D plan sponsors and their PBMs handle them.
CMS is considering requiring the negotiated price at the point of sale to reflect the lowest possible reimbursement that a network pharmacy could receive from a Part D sponsor for a covered drug.
The price reported at the point of sale would include all price concessions that could potentially flow from network pharmacies as well as any dispensing fees. The negotiated price at the point of sale would exclude any additional contingent amounts that could flow to network pharmacies and increase prices over the lowest reimbursement level. If a pharmacy is paid an amount above the lowest possible contingent incentive reimbursement, the difference between the negotiated price reported to CMS and the final payment would be reported as negative DIR.
IMPACTS. Given the growth in rebates especially relative to increases in Part D payments - premiums, subsidies and cost-sharing - it would appear that rebates are having more than just an impact on Part D premiums. What has become a massive transfer of revenue from drug companies to Part D plan sponsors and their PBMs, could also be playing a role in financial performance of the Part D sponsors and their PBMs. A diversion of some portion of the $25 billion in 2015 rebates to Part D beneficiaries will likely have a negative effect on CVS, HUM and UNH which collectively have more than half of the Part D market share.
Since the weighting of rebate amounts will enhance the influence of high price-high rebate drugs on the amount passed through to Part D enrollees, there will be a corresponding incentive for plan sponsors to encourage lower cost alternatives when available. Top selling name brand drugs which have been shielded from generic and biosimilar competition because of the rebate-formulary feedback loop may be at risk.
Normally we would be inclined to think such a radical departure from the status quo would get buried by lobbyists. However, the Trump administration is clearly coming down hard on the side of saving Medicare beneficiaries money even when it means disrupting the entire PBM/Part D industry.
We would look for an official proposal from CMS in early to mid-2018.
Call with questions.
Emily Evans
Managing Director
Health Policy
@HedgeyeEEvans
