
This afternoon, CMS released the CY 2018 payment update for home health agencies and proposed for CY 2019 a change in the payment system to the Home Health Groupings Model in CY 2019.
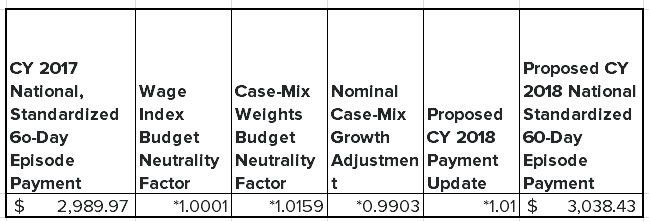
The payment update is uneventful due to the CY 2018 override provided by Congress which we discussed here. The national, standardized 60-day episode payment will increase as follows:
We went through the esimated impact of the Groupings Model on AMED, LHCG, KND and HLS here. In June, we did not anticipate a proposal this year but we revised that view as the Trump administration demonstrated a pretty aggressive rulemaking posture over the last several weeks.
The main features of the Groupings Model are:
-
Episode length is reduced from 60 days to 30 days.
-
The 30-day episode payment will be determined by first calculating what would be the CY 2019 60-day episode payment, adding in what would be the NRS conversion factor and dividing by two.
-
As is the case today, episode payments would be classified as early or late. Unlike the current system, only the first episode – not the first and second – would be an “early” episode.
-
Each episode would be differentiated based on admission source – community or institutional – depending on what health care setting was used in the 14 days before admission to home health.
-
After determining timing of episode – early or late – and admission source – community or institutional – the HHGM would classify the episode into six clinical groups based on the principal diagnosis.
-
The episode would be further classified based functional level and presence of co-morbidities.
-
Therapy services would eliminated as a payment factor.
CMS is proposing to implement the HHGM in a non-budget neutral way, which is surprising. CMS generally likes to implement major payment changes with a long glide path. Knowing full well they will get significant blow-back for a non-budget neutral implementation, CMS is also considering applying a partial budget neutrality factor in CY 2019 alone or over several years.
Our analysis of the impact of the HHGM payment system was predicated on the assumption that the model would be implemented in a budget neutral manner. Home health agencies, whose reliance on therapy is in line with national means like AMED, would certainly have to make some adjustments but would not have been too negatively impacted by the change.
However, implementing the HHGM in a non-budget neutral manner will reduce overall home health payments by about $1B in CY 2019 – a 4 percent reduction. We believe CMS will have to back-off the non-budget neutral implementation but even a partial budget neutral implementation will reduce overall payments by an estimated $480 million.
It is important to know that the impact estimated by CMS assumes no change in utilization patterns, which is unrealistic. There is no area of Medicare that adapts to changing payment circumstances like the home health industry. We would expect that trend to continue and the actual impact will be mitigated by changing practice patterns.
The real losers will be contract therapy companies. When the HHGM is combined with the new SNF payment system uncer consideration, the outsourced therapy industry is probably in for some real heartburn in the next six to nine months.
Call with questions.
Emily Evans
Managing Director
Health Policy
