
Ozempic has become health care's inverted AI, to watch the tape yesterday. At this point, it seems poised to solve America's fiscal crisis by curing everything from heart disease to diabetes, whilst ending our love for Cheetos and Pepsi-Cola. That would all be nice, of course, but not very likely. The hype on weight loss drugs says more about the bleak outlook for bio-pharma (and NVO's astute manipulation of our mood these days) than it does its implications for the health care system.
DVA was one name that got the Ozempic/Wegovy treatment yesterday after NVO released a vague-ish presser on their FLOW study, looking at the effect of semaglutide on kidney outcomes in participants with Chronic Kidney Disease and Type 2 Diabetes. The company stopped the trial due to efficacy and will publish a read-out in 1H 2024.
The first response to that result should be 'duh." If a drug controls diabetes, it will also limit its significant negative knock-on effects. The second response should be that Ozempic may already be having a negative effect on dialysis volumes. After all, it has been on the market since 2017. It is widely prescribed and has a robust Direct-to-Consumer presence.
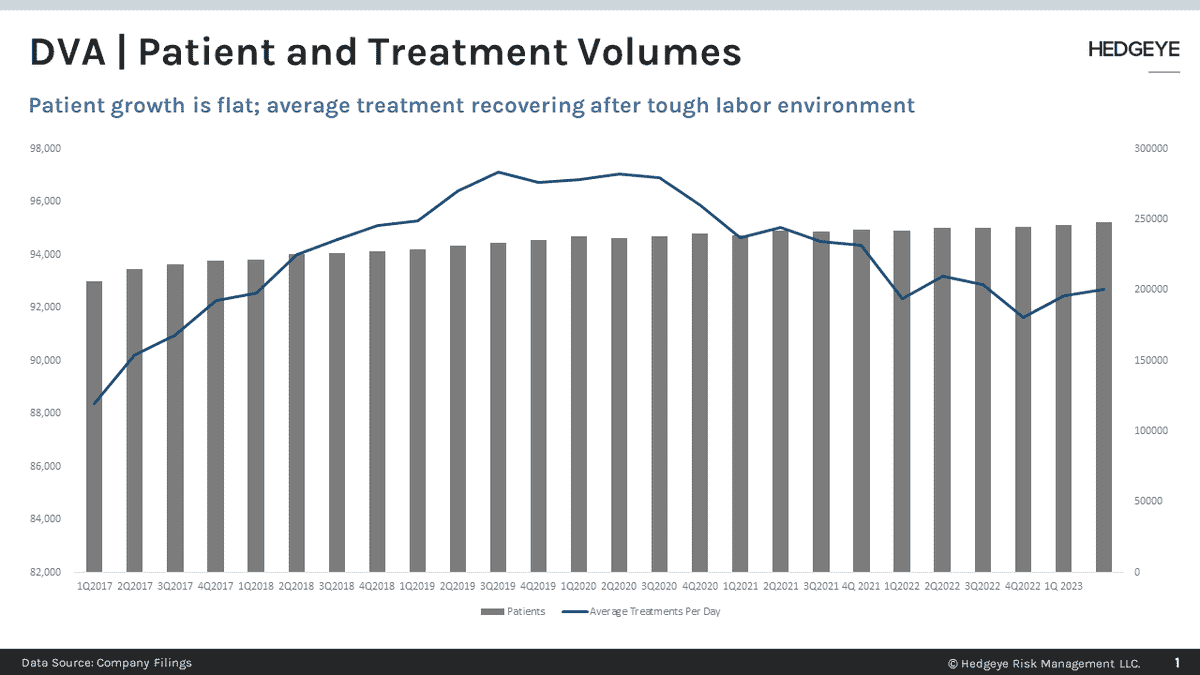
Meanwhile, as obesity and T2D prevalence has increased, DVA patient volumes have flatlined while average treatments per day have dropped. Some of that result is due to Covid which disproportionately affected the ESRD population and drove the incidence rate from 387 to 363 per million from 2019 to 2020. Some of that is likely due to population-wide demographics. The incidence rate reached its peak in 2005 at 4.31 per million and it has been mostly downhill since. Hence the extreme concentration of the industry.
Most certainly, better treatments for diabetes and other comorbidities, like Ozempic, are also having an effect. This progress may be due in part - although a little early to call it - the expansion of Medicare Advantage coverage to include ESRD in 2021. Generally speaking, CMS under-reimburses MA for ESRD patients and the effect of underpayment is a concerted effort to divert patients from a dialysis fate.
(See Monogram Health as a great example of that effort.)
Of course, the patients most likely to benefit are those engaged in their health. Sadly, many people end up on dialysis because they crash into an emergency room and encounter the warped incentives of the dialysis industry. Those outcomes are not likely to change but it is a poor foundation for the future of DVA.
Let me know what you think.
Emily Evans
Managing Director – Health Policy
Twitter
