


Update: Late yesterday afternoon, one of the Capitol Hill newspapers, Inside Health Policy, reported basically what we did, reaching pretty much the same conclusion. Later yesterday afternoon, CMS issued a statement: “We have not announced a change in timing and we continue to review comments." CMS claims that the date of March 2019 was simply the latest date they could finalized the proposed rule without starting over. According to IHP, "A CMS official told IHP that 'Final Action' on the White House Office of Management and Budget's website in this case reflects the statutory deadline for a final rule, not the expected time to issue a final rule. IHP goes on to point out: "However, the statutory deadline and the final action dates listed in the agenda for many rules are not the same."
We share IHP's skepticism and think the proposal has problems - real problems not just political problems - with oncologists, rural providers, non-profit hospitals, patient advocates and others. Time will tell.
Drug prices have become a white hot political issue this year and for good reason. In October, 2015, a Kaiser Family Foundation tracking poll found that respondents felt affordability of prescription drugs was a top health care priority. In a March report from the Health and Human Services Office of the Assistant Secretary for Planning and Evaluation (ASPE), the research arm of the department, estimated that in 2015, Americans spent $328 billion on retail (drugs sold at outlets that serve patients like Walgreens and CVS) and $128 billion on non-retail (drugs dispensed through physicians offices). Drugs accounted for 16.7 percent of all health care spending in 2015.
The ASPE found that, after a period of slow growth from 2008 to 2013, retail and non-retail drug spending dramatically increased in 2014. Chart 1 illustrates recent drug spending and projections from the HHS Office of the Actuary.

Source: ASPE
A driver of the increased spending appears - though there is some conflicting data - to be increased costs associated with the use of specialty drugs. ASPE estimated that 30 percent of the increase in drug spending in recent years is attributable to escalating prices. Other factors include an increase in prescriptions per person, general population growth and economy-wide inflation.
These facts took human form in late 2015 when the tone deaf Martin Shkreli, former CEO of Turing Pharmaceuticals, created a stir by raising the price of Daraprim, a drug for which Turing had recently acquired the manufacturing license, and earned him the title of "most hated man in America." The drug industry's standing in the court of public opinion was further eroded by the bad behavior of Valeant Pharmaceuticals (VRX) and a spate of tax inversion deals. The combination of a real and dramatic increase in drug costs and the convenient arrival of a boogie man, forced the issue onto the 2016 Presidential campaign platforms. In October 2015, Senator Bernie Sanders released his plan for combating the increase in drug costs and was quickly followed by Secretary Hilary Clinton. Donald Trump appears to also be considering ways that drug prices can be controlled.
The confluence of events and the predictable political response had quite a few people wondering if the time was right for federal intervention to control drug prices. Some of those people were at the Center for Medicare and Medicaid Innovation and the White House. In early March, the Obama Administration, out of the blue, proposed the Part B Drug Demonstration. The proposal had not previously appeared on the Obama administration's regulatory agenda suggesting that they were exploiing a political opportunity so in the waning years of their administration they could claim some credit for reform of drug prices.
We were not among those who saw federal intervention in the drug price issue as viable. The reimbursement system for drugs is too complicated and too connected to the payment systems for physicians and hospitals to be easily altered. Furthermore, the drug industry lobby's power and effectiveness in Washington is legendary. Our money was on Pharma and on Friday the Obama administration offered pretty compelling evidence that the Part B Drug Demo was not moving forward anytime soon. The Spring 2016 Unifed Agenda - a "honey-do" list of regulatory activities in the coming months - includes the Part B Drug Demo but with a finalization date of March 2019. Since the Demo cannot move forward until the rule is finalized, it would appear, assuming there has not been a clerical error, the project will be backburnered until the next Administration. The next President can proceed or abandon the whole thing.
What Are Part B Drugs?
Medicare pays for prescription drugs obtained from retail pharmacies through the privately administered Part D plans. Drugs administered in physicians’ offices and Hospital Outpatient Departments (HOPDs) (e.g. chemotherapy infusions) are reimbursed through direct payment to doctors and hospitals via Medicare Part B. Many of these Part B drugs are what the ASPE referred to as "non-retail" drugs. The Medicare payments to doctors and hospitals are comprised of both reimbursement for the drug itself and payment for the administration of the drug either through the physician fee schedule or the Hospital Outpatient Prospective Payment System (OPPS). It should be noted that reimbursement for services on the HOPD schedule is considerably higher – 20 to 30 percent in some cases- than the physicians fee schedule.
Medicare reimburses for Part B drugs by inflating the Average Sales Price from manufacturers to wholesalers by 6 percent. This formula takes into account all rebates and discounts offered by the manufacturer but not “prompt pay” discounts that are not typically passed on to the provider. Part B drug reimbursement has been subject to sequestration for the last several years and that is scheduled to continue until 2024. The impact of sequestration on reimbursement is -1.6 percent so that the effective reimbursement is ASP plus 4.4 percent.
The Part B Drug Demonstration
The Part B Drug Demonstration would be a five-year, mandatory program with two phases that would significantly upend Medicare Part B payments. Phase one of this experiment, as it is often called due to the inclusion of a control group, would have begun in Fall 2016. The current reimbursement system of Average Sales Price (ASP) of the drug plus 6 percent would be replaced by ASP plus 2.5 percent (0.9 percent after sequestration) plus a $16.80 flat fee. All physicians and Hospital Outpatient Departments (HOPD) would be required to participate. However, roughly half would be part of a control group.
Phase two of the Part B Drug Payment Model would have begun in early 2017 and layered on top of the phase one payment method a veritable smorgasbord of Value-based Purchasing (VBP) payment tools. CMS has provided relatively few details on phase two. They do propose that the VBP could include:
- Reference Pricing – Payment for a drug would be based on the price of all therapeutically-similar drugs. A reference pricing scheme could be based on the average price of all drugs in the group or on the lowest drugs in the group. Because of a prior and quite negative experience, CMS has stipulated that any reference pricing scheme would not include increased beneficiary liability.
- Indications-based Pricing – Under this approach, Medicare payment for the drug would be based on safety and cost-effectiveness of different indications. In other words, Medicare would pay a higher reimbursement for a drug meant to treat conditions for which research shows greater effectiveness and less when the drug is used on conditions where the drug is less effective.
- Outcomes-based Risk Sharing Arrangements – CMS would enter into agreements with manufacturers to provide price adjustments when products do not meet specific targeted outcomes. Commercial insurers have been experimenting with this approach in recent months and it has been heralded as a private sector approach with promise.
- Discounting or eliminating patient cost-sharing – Medicare would provide incentives to patients that use “high value” drugs by limiting cost-sharing.
- Clinical Decision Support – CMS would provide online tools to provide education and literature to physicians and a feedback mechanism for prescribers to provide data on claims and utilization.
The Part B Drug Demonstration model would consist of four populations:
- A control group paid using the existing Medicare reimbursement formula of ASP plus 6 percent
- An experimental group using the existing payment formula of ASP plus 6 percent and the VBP tools
- An experiment group using the new payment formula of ASP plus 2.5 percent plus the flat fee of $16.80 flat fee
- An experiment group using the new payment formula of ASP plus 2.5 percent plus the flat fee of $16.80 and the VBP tools.
If the details of phase one seem a bit arbitrary and those of phase two rather vague, you are not alone. Aside from a MedPAC study last year where the 2.5 percent add-on was presented as merely an illustrative example, and chosen because it was higher than the 1-2 percent reportedly given to wholesalers, there does not seem to be much research to support its use.
Phase one also fails to even address the problem identified by CMS. In the studies released in conjunction with the Part B proposal, CMS characterizes the problem as one where providers have little incentive to prescribe lower cost, but equally or more effective drugs when they are available. As noted above, a big part of spending increases are attributable to specialty drugs. There is not yet an agreed upon definition of a specialty drug but most people agree they usually are manufactured or produced by a single company implying there are no alternatives. Yet the phase one proposal makes no distinction between reimbursement for drugs with comparably effective alternatives and those without. Given the history of Medicare, where reimbursement cuts are inevitably met with margin protection through higher utilization, the phase one proposal could actually create incentives for increased prescriptions for drugs without alternatives.
Phase two of the proposal is significantly more nuanced but treading dangerously close to charging Medicare with a role in determining cost effectiveness of drugs – a dog whistle for patient advocates and often used as code for rationing of care. This phase does include opportunity to tailor incentives for providers. However for things like indications-based reimbursement, CMS would need to rely on some scientific knowledge-base that is undisputed. There is a significant lack of detail and specifics on how exactly, CMS would measure things like effectiveness and outcomes making phase two look unready for prime time.
In short, phase one appears to be more complete than phase two but arbitrary and an oversimplified response to an extraordinarily complex problem. Phase two is less defined but equally inadequate in addressing the multi-faceted and complex nature of Medicare Part B drug spending.
The Drugs.
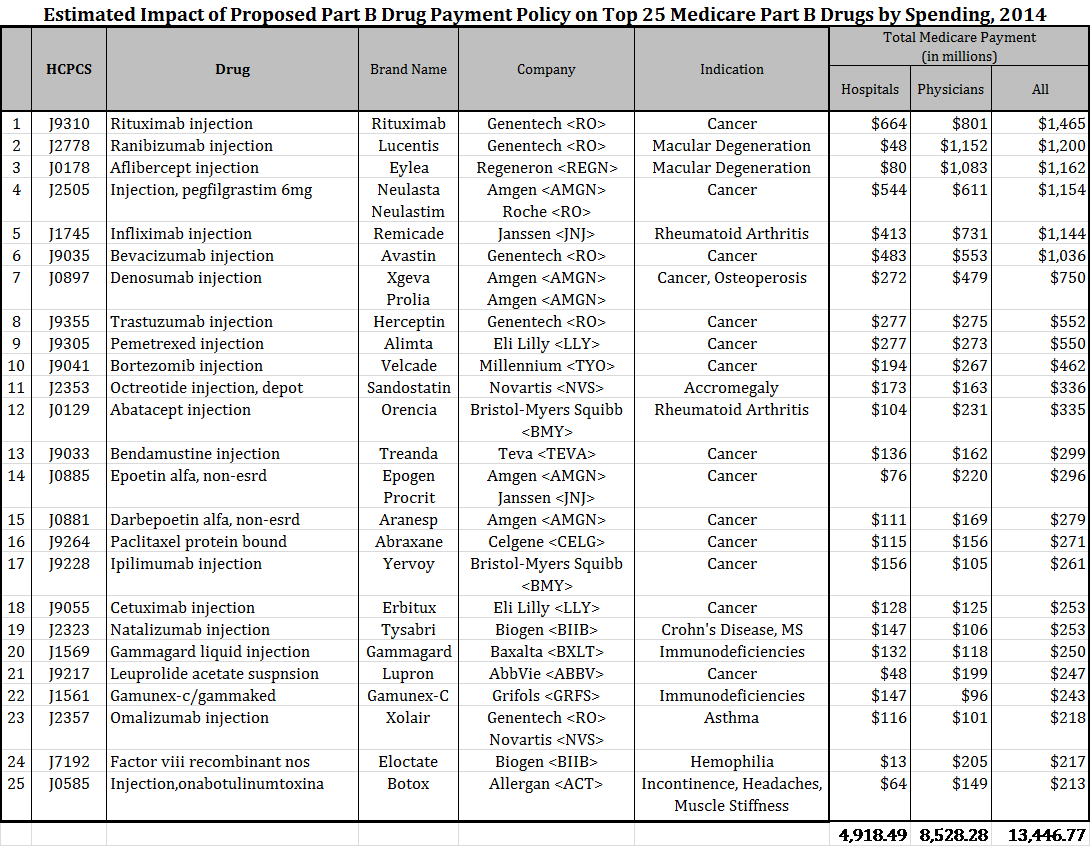
The Part B Drug model is budget neutral – meaning CMS anticipates paying the same amount of money, in aggregate, to physicians and HOPDs as they would had the program not been implemented. As such, some practice areas will see an increase in payments for Part B drugs, while others will see a decline. Anesthesiologists, for example, will see an increase in Part B drug reimbursement while oncologists will see a decrease. This result is not a surprise since drugs administered by oncologists, ophthalmologists and rheumatologists usually make the list of Top 25 drugs for Medicare spend.
Topping the list of most Medicare dollars spent is Roche's Rituxan to treat certain cancers and Lucentis to treat Macular degeneration.
CMS claims - and we have no reason to dispute it - that there are many oncologists for whom half their income is derived from the drugs the prescribe. The finding appears to be their sole justification for structuring the program in such a way as to alter provider compensation.
The Implications. The near term implications for physicians and patients was significant and the source of much of the opposition to the program. While the Obama Administration was able to keep its party on the reservation for a hearing last week on the Demo, members of both parties raised objections. Opinions ranged from Republican calls for a complete withdrawal to requests from Democrats to downsize the project. In these days of a divided Washington, it is tough to find such consensus.
Driving the debate was the Pharma who understood this Demo for what it was: a political response to a very complicated and difficult problem. Political reactions call for more politics not less. Pharma put together a coalition of physicians, hospitals and patients to be the face of the opposition who effectively pointed out the many flaws of the program. After a week of floating trial balloons suggesting a much smaller Demo was in the offing, the Obama Administration released the Spring 2016 regulatory agenda. Finalization of the Part B Drug Demo is now scheduled for March of 2019.
The delay is good news for Pharma who apparently still has what it takes to protect their interests. Because of that, efforts by the next President to "do something about drug prices" will not be easy. Pharma's success in beating back this threat however, did rest solely on their lobbying prowess. The fact is that federal drug reimbursement policy has created a web of interests that are tough to unwind. Part B drug reimbursement is an element of physician compensation and not simply a cost recovery system. Non-profit hospitals that increasingly derive significant portions of their annual revenue from the 340b drug discount program want to avoid any disruption of the current system of reimbursement. Had Pharma failed at blocking the Part B Drug Demo, interests favoring drug price regulation would have had the toehold they needed for additional intervention. In political terms, the Pharma lobby would have suffered a loss that would have called into question their ability to defend the industry, a weakness that would have been exploited by supporters of price controls.
Any changes to how the federal government reimburses and controls drug prices will be a hard fought fight and it doesn't look like anyone is spoiling for that just yet.
