|
Editor's Note: This is a complimentary research note published by Healthcare Policy analyst Emily Evans on 2/21/21. CLICK HERE to get COVID-19 analysis and alerts from our research team and access our related webcasts. |

Politics
It varies from place to place, but most laws passed by state and local legislatures end with some version of “the health, safety and welfare of the people so requiring it.”
It serves as an almost daily reminder that the authority conferred upon states to legislate flows from the constitution’s 10th Amendment, “the powers not delegated to the United States by the Constitution, nor prohibited by it to the States, are reserved to the States respectively, or to the people.”
As American politics has become nationalized, some governors are quick to cast envious looks at 1600 Pennsylvania Avenue. Those powers delegated to the federal government have become much more interesting than, say, keeping the power on, the schools open and the public health apparatus fully operational.
In an uncomfortably large number of states, chief among those, California, mayors and governors have ignored their primary responsibilities.
Neglect of the basic and decidedly unglamorous duties of state and local governance has put California Governor Gavin Newsom in a bit of a pickle. On Friday the Secretary of State released an update on the gubernatorial recall effort. As of Feb. 5, organizers have submitted about 1.1 million signatures of which 800,000 have been reviewed. Of the 800,000 reviewed, 670,000 or 84% have been deemed valid.
An error rate of less than 20% is considered by those with recall experience (don’t ask) to be ideal. Organizers claim they have collected 1.7 signatures, suggesting the effort may be less than 100,000 shy of its goal with about three weeks before the March 16 deadline.
Let us pause and note that recall efforts are exceedingly difficult, these numbers notwithstanding. The most challenging aspect is finding someone who can beat the incumbent subject to the recall.
Whatever the outcome, there is certain to be some impact on the politics of pandemic in California and beyond. The common cause formed with groups like educators’ unions, who shared Newsom’s objective of allowing the state economy to slumber on until the White House’s occupant was turned out, are not going quietly back to work. An operational school system is a prerequisite for getting women back to work – many of them critically needed health care workers. (AMN)
With no foil in the White House and opportunities to blame its previous occupant quickly receding, the clock is ticking on pulling it together at the state and local level. It is also a good reminder that electing a Governor is not the same as elected a president.
Policy
This week President Biden is expected to nominate Chiquita Brooks-LaSure as CMS Administrator. HHS Secretary nominee, Xavier Becerra, is scheduled for confirmation hearings as well.
Both have long tenures in the health insurance-centric policies that characterized the Obama administration. For that reason, they are safe choices.
At least for now.
Like earmarks that are being resurrected, a health policy that focuses solely on health insurance instead of health, has a certain dogeared-ness to it. The emerging power of a younger generation who were so badly mistreated by the ACA’s provisions (except that part where kids get to stay on mom or dad’s insurance until 26) are understandably skeptical of continuing down that road.
At some point in the not-too distant future the policy paths will diverge with a very left leaning cohort demanding universal coverage and the rest looking for simple, frictionless ways to obtain health care at a reasonable price.
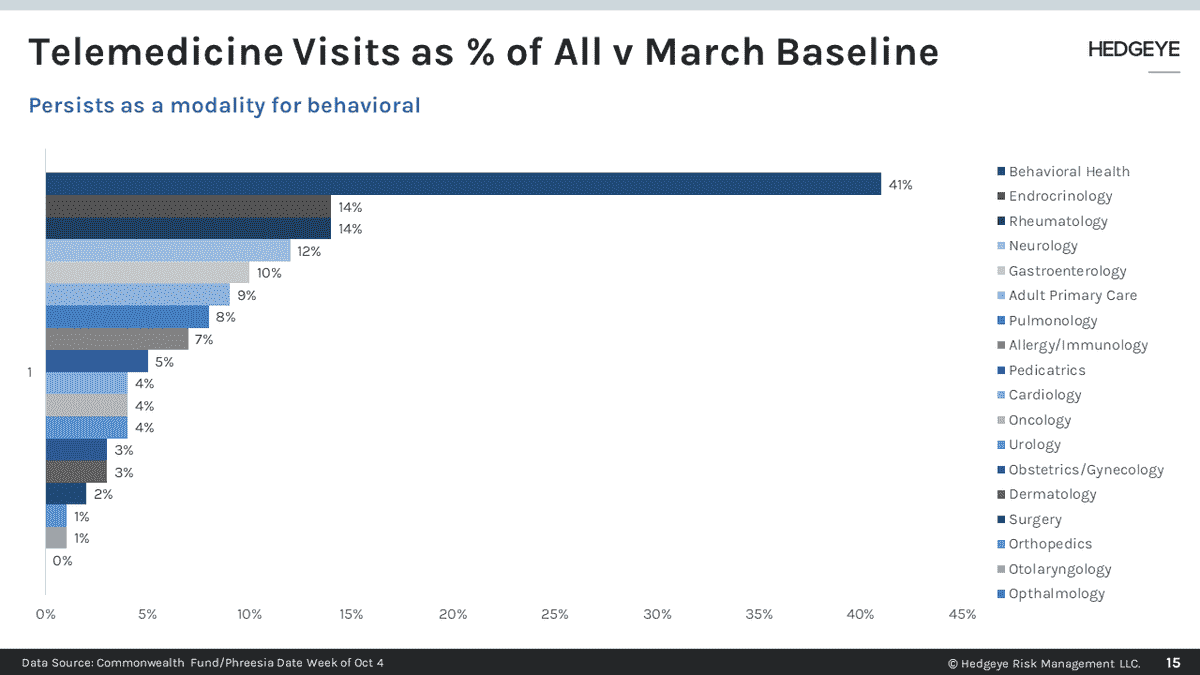
There is no clearer demonstration of who is likely to prevail than how behavioral health has been transformed not just by the COVID pandemic but by the people using it.
Unlike the delivery of physical health, treatment for mental health and substance abuse has largely operated outside the insurance system. Even in the face of federal parity requirements, inpatient coverage has been limited. Outpatient providers, when they are available, usually refuse to go in-network because the reimbursement is so low. The geographical dispersion of therapists skews toward urban centers.
Enter pandemic. Unlike medical doctors, therapists, psychologists and social workers are trained to talk more than to touch. For these practitioners, the last year was an opportunity to expand the practice of behavioral health for a generation facing more challenges than any since the Great Depression. Unlike their great grandparents, for the last cohort of the last century, the stigma for mental health treatment has melted away.
While insurance carriers are likely to slowly move telemedicine coverage back toward pre-pandemic norms, their reach will not extend to behavioral treatment. Having operated mostly on a cash basis for years and now finding new acceptance, teletherapy is here to stay. (TDOC)
Easier, cheaper and faster wins every time and now in health care.
Power
Since Gannett started rolling up local newspapers in the 1990s state and city-focused journalism has been on a long, slow slide to irrelevance.
Legendary local dailies like the Louisville Courier-Journal and the Nashville Tennessean, aided and abetted by the adtech machinery of Google that ultimately destroyed their business model, have found themselves in competition with cat videos, conspiracy theorists and vacation pictures from your high school friend’s vacation.
As local papers pursued all the tales that yield them the clicks and likes necessary to satisfy the algorithmic gods, they missed a once in a lifetime opportunity to write the first draft of the COVID-19 pandemic’s history and ultimately to shape solid public policy.
The failures of the COVID response rest as much at the state and local level as they do with the federal government. Yes, it was a major misstep in the federal response to stall approval of testing protocols.
The shortage of testing materials and PPE also can be laid firmly at the feet of Washington’s bureaucracy who ignored years of warnings about the supply chain’s fragility and depleted stockpiles.
The uneven vaccine rollout, something that can only be engineered at the local level through a complex cooperation between distributors, health departments, providers, community organizations, and in some cases the National Guard, demonstrates that a good number of local leaders have failed to meet their most basic responsibilities as well.
Funding, of course, has played a role. Public health – when we are not talking about Medicaid expansion or another nationally recognized priority – was until spring of 2020, of little interest. Disrupting that narrative, however, is the reality of the math. Pure public health funding has increased a bare 1-2% a year for the last decade or so while property values and sales tax revenues have soared. There is no getting around the fact that for many local leaders, public health was simply not a priority.
Which brings us the second problem. The politics of many of America’s urban centers and a few states are controlled by poorly conceived term limits premised on two false notions; that any problem governments face from poverty to energy can be addressed in eight years or less and; officials turned out by term limits will go back to their civilian lives.
Both are demonstrably false.
Local leaders needing to solidify their reputations to secure the next office met reporters told to “think big” by their editors. What should have been inquiries into poor data infrastructure, absent interventions with at-risk populations, and lack of preparation were reduced to public shaming of gatherings and other resistance to nonmedical interventions that fit nicely into a national narrative.
The Biden administration has proposed new funding for health care workers, data collection and disease surveillance all of which will be welcomed at the local level.
But money was never the problem.