
|
Editor's Note: This is a complimentary research note published by Healthcare Policy analyst Emily Evans. CLICK HERE to get daily COVID-19 analysis and alerts from our research team and access our related webcasts. |
Politics
Politics is a high contact, blood sport and Texas Governor Greg Abbott knows how to play the game.
For the last several weeks, the Texas Medical Center in Houston has been posting daily updates on COVID-19 hospitalizations and, importantly, projections on available floor and ICU beds. Like the IHME model at the University of Washington, TMC's capacity projections assume historical utilization would not be affected.
In other words, there would be no regulatory or behavioral interference with medical procedures that can be deferred or performed in another setting, thus freeing up hospital space. Given recent experience in New York, it is a rather far fetched assumption.
Elective procedures are, of course, where hospitals make their money. So the TMCs' modeling may be more about the system's financial statements than realistic estimates of hospital bed capacity. Their dire outlook had the desired effect. Political leaders and the Texas press, citing the TMC data as evidence the Texas health system would be over-whelmed with COVID-19 victims, called for a restoration of stay-at-home orders and other restrictions on commerce and assembly.
As a bonus for his political opponents, Gov. Abbott's competency over resisting these measures comes into question; allowing them to draw a straight line from Washington, DC to Austin, TX.
Voila! Texas hospitals shift the risk of COVID onto businesses and individuals all while preserving margin enhancing elective procedures.
Gov. Abbott is having none of it. On Friday, he issued an Executive Order suspending elective procedures at inpatient hospitals in Texas. Included in the order was this valuable hedge:
|
[P]rovided, however, that this prohibition shall not apply to any surgery or procedure that, if performed in accordance with the commonly accepted standard of clinical practice, would not deplete any hospital capacity needed to cope with the COVID-19 disaster. |
In other words, the Governor is allowing things to carry-on as before but with a threat that elective procedures will end the moment he deems it necessary.
HCA and other Texas hospital promptly moved to assure patients that it was business as usual:
|
After reviewing the order and the implications to our patients, it is important to know that at this time our hospitals have the bed capacity, supplies and equipment we need to continue serving patients, meeting the requirements under Governor Abbott’s executive order. Beyond our hospitals, we also have alternate settings for surgeries, including surgery centers and specialty hospitals, which also factors into our decision to schedule a surgery. |
Nonetheless, Gov. Abbott's message of "pipe down, do your job and leave crisis management to me" was received loud and clear. The TMC has removed their bed capacity reports from their website.
Policy
Late on Friday, the White House Coronavirus Task Force held a briefing to discuss the latest outbreaks in the South, Southwest and Eest and offered a small but hopefully sign that more traditional public health strategies may finally be taking root, although not without some challenges.
Epidemics tend to evolve over time. Assumptions made early in an outbreak must be revisited. For example, our understanding of COVID-19's mortality rate was informed by the experience of countries that lack much of the U.S. health system's capacity and expertise, leading to some faulty model assumptions and, in turn, to some disastrous policy decisions that unleashed COVID-19 on nursing homes in the Northeast.
As testing has expanded from the health setting to the community and more - many, many more - cases are identified that represent little in the way of clinical demand, the role young people are playing in disease spread is becoming more clear.. As cases have exploded in California's Imperial Valley and other agricultural areas, migrant workers and new Americans are becoming a focus.
We have never seen "shut-downs" as a durable strategy for any president, governor or mayor other than as a way to prepare the health system. Use of that tool across the U.S has lead to an unreasonable expectation that the disease could be eliminated and COVID-19 would just be a bump in the road.
The facts are the tried and true approach for the last century has been case managment, combined with education of communities most likely to be affected and a repeatable and consistent public health message.
On the first two prongs, some progress is being made. The CARES Act poured a lot of money into states to augment their existing contact tracing programs. There have been reports of labor shortages and, as cases grow in places like Texas, the system can get stressed. Immigrant and migrant communities as well as people living in poverty are often wary of answering a phone call from the government.
Actually finding contacts for each case, however, is only part of the system's value. The other is the data and information collected yield a better understanding of who gets infected, under what circumstances, who they pass it on to and who eventually needs clinical care.
That information, in turn, can be used to identify community groups who have the trust of affected populations and can educate about risky behaviors and necessary interventions. As Dr. Fauci pointed out on Friday, this approach has been used to contain AIDS, here and around the world.
On the last prong, there is a long way to go. Science evolves. Data gets collected; evidence gets developed; theories change; and new approaches emerge. In our puritanical "I told you so world" there is little tolerance for these divergences.
A good public health message is designed to be credible but flexible enough to accomodate the evolving nature of the science. It also needs to be translated into terms the affected community understands.
In the case of a key driver of spread - young people - you can understand their confusion. They were told they could not get sick. Then they were told to stay home but then that they should go to protests. Then they were told to be tested but not told to self-isolate. So they went out for a drink with friends.
The White House, the CDC and local governments are starting at zero with a group that poses the most pressing challenge for disease containment.
Power
The Governors of Texas, Florida and California are now limiting bar service as a strategy to contain the spread of SARS-CoV-19 among the young. This move represents the evolving understanding of the disease Dr. Deborah Birx alluded to in the White House Task Force briefing on Friday.
After congregate living arrangements, social activities are a risk for infection.
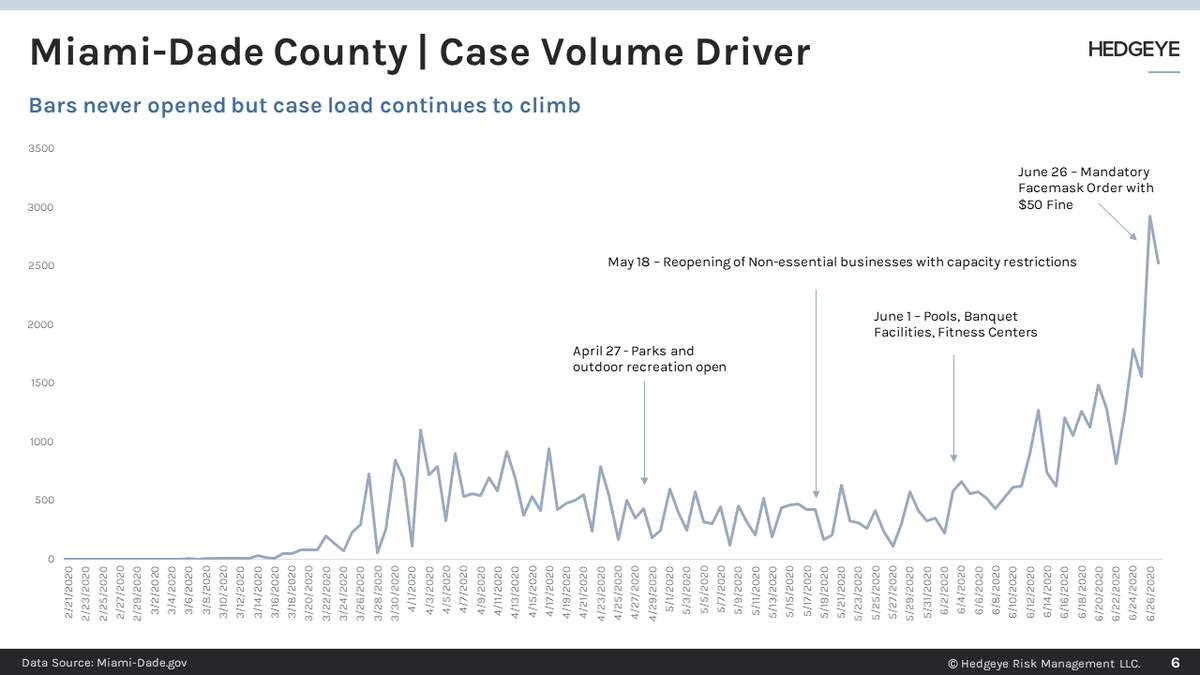
Unfortunately, it is far from clear closing bars will be an effective intervention. Miami-Dade has never re-opened them, yet the county remains a hot spot. What may be more a factor are social gatherings at homes.
A recent letter from one Florida Mayor implored his constituents to stop with the house parties. Governor DeSantis noted, in response to a question about mask wearing that the problem was young people partying and Florida's solution was to deliver a clear and concise public health message of avoiding the 3-Cs: closed spaces, crowded places and close contact.
What closing bars does do is send a message that there are consequences -albeit indirect - for not following the rules. That may get the infectious young's attention but there better be some clearer instruction on what to do next or speakeasies are going to make a comeback no one predicted.
