
On Friday, CMS released the first of the 2020 payment rules for Hospice, Inpatient Psychiatric Facilities, Skilled Nursing Facilities and Inpatient Rehabilitation Facilities.
Hospice. CMS had several unpleasant surprises for the hospice industry. First, it decided to act on a long- standing concern about low utilization and access to three levels of hospice care: Continuous Home Care, Inpatient Respite Care and General Inpatient Care. Approximately 98% of hospice days are delivered through Routine Home Care.
CMS has reported in the past that many home hospice agencies have claimed no days with any other service, leading the regulators to believe many hospice agencies do not or cannot provide care in these settings, contrary to Medicare Conditions of Participation.
To address the issue, CMS is proposing to drastically increase payments for CHC, IRC and GIP:
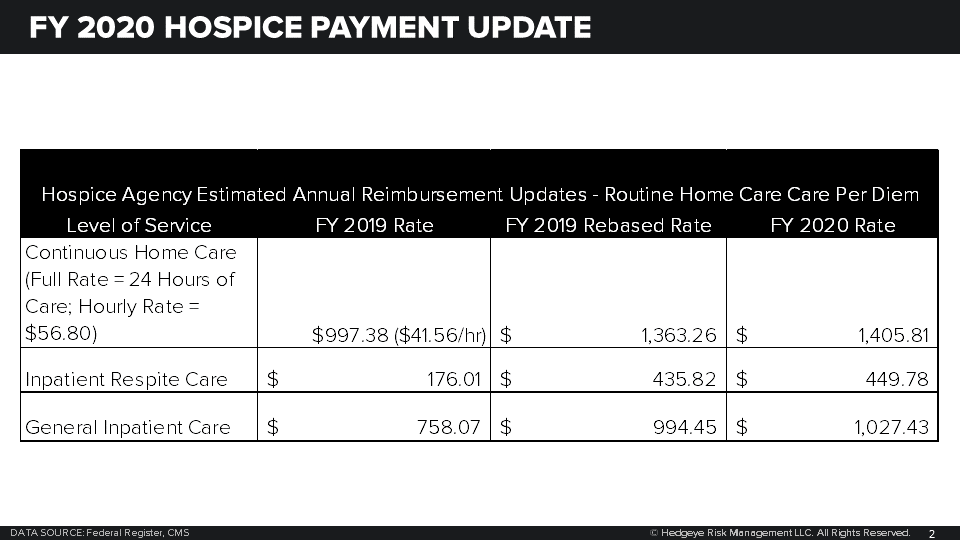
Unfortunately, to achieve budget neutrality, CMS is also proposing to reduce the rates for RHC. A 2.7% cut is being applied to the FY 2019 rate which, is then inflated with market basket and other adjustments to achieve the FY 2020 per diem. The result is a reduction in the per diem payment in FY 2020.

It is very important to note that CMS’s research indicates that Medicare is paying approximately 14% more than cost for RHC days, suggesting the RHC rate could be reduced further to accommodate additional increases in CHC, IRC and GIP days, expecially if utilization of these services remain low.
The second unpleasant surprise is that CMS is seeking comment on how hospice service can be better integrated with other care. To that end they are seeking comment on the addition of hospice services to Medicare Advantage plans through CMMI or otherwise.
One of the program integrity challenges identified in several False Claims Act lawsuits and in Medicare rulemaking is that the hospice benefit is often abused and used to provide services to people who may not be eligible. Given the passive nature of Medicare FFS – providers submit bills and get paid frequently with few questions asked – the introduction of a care manager will create a very different dynamic for the industry.
The hospice payment cap is proposed to increase by 2.7% from $29,205.44 to $29,993.99
Total payments are expected to increase $540 million, most of it in the form of higher payments for CHC, IRC and GIP levels of service.
Inpatient Psychiatric Facilities.
Payments to IPFs are expected to increase $75 million in FY 2020. Other than a payment increase of 2.63% and some adjustments to quality measures and other program items, the rule contains no surprises

Inpatient Rehabilitation Facilities. Payments to IRFs are expected to increase $195 million in FY 2020, largely due to an almost 3.5% payment increase.
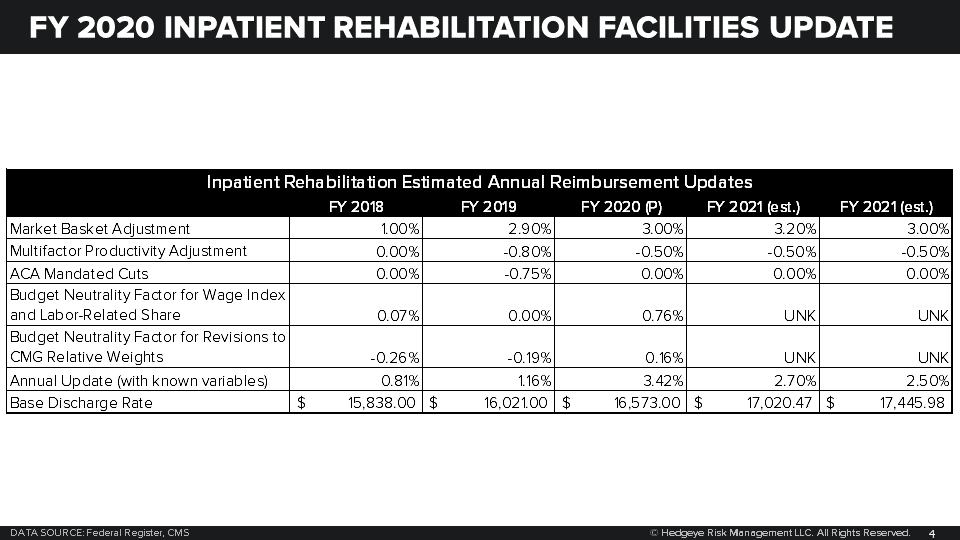
The outlier threshold will similarly increase from $9,402 to $9,935.
Skilled Nursing Facilities. FY 2020 SNFs will be under a new payment system called the Patient Driven Payment Model. This payment model de-emphasizes therapy as a payment factor while increasing payments for nursing care.
Payments to SNFs are now divided int o six components, five of which will be case-mix adjusted.
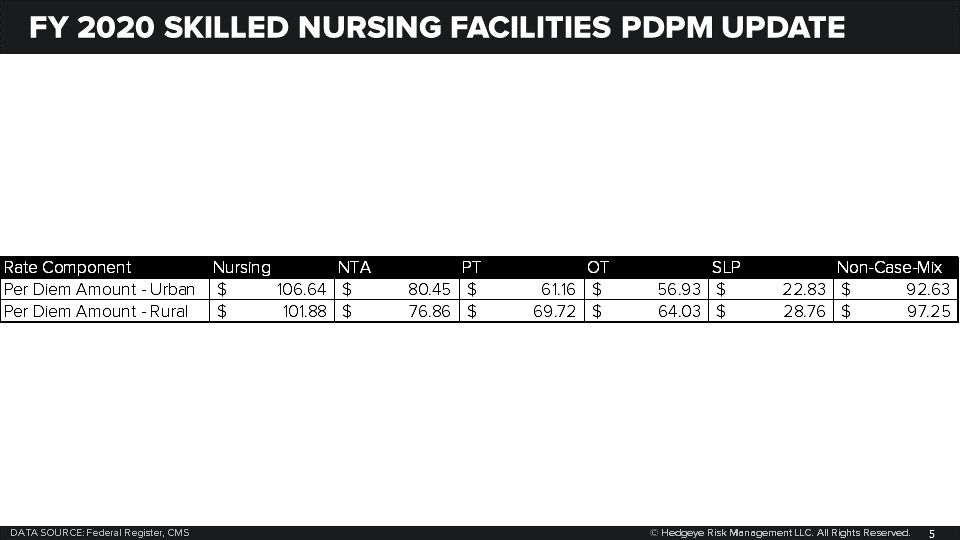
Overall payments to SNFs are expected to rise $887 million in FY 2020.
Call with questions. CMS has finally figured out how to write a Medicare rule with less than 250 pages so we have all the time in the world.
Emily Evans
Managing Director – Health Policy
Twitter
LinkedIn
