Sen. Kamala Harris launched her 2020 presidential bid over the weekend at a rally in Oakland, CA, including Medicare-for-All in her platform and signaling the persistence of that message in most, if not all Democrat campaigns throughout 2019 and 2020.
Medicare-for-All has different meaning depending on who is talking. The range of policy possibilities is wide. At one end is a single payer system where employer-based insurance is, in effect, prohibited and Medicare FFS, Medicare Advantage and Medicaid are replaced with a single government payer. At the other end of the spectrum are optional buy-in programs to existing Medicare and Medicaid.
In the last Congress, there were eight bills filed that fit into that range of possibilities. There are:
- S. 1804 Medicare for All Act of 2017
- H.R. 676 Expanded and Improved Medicare for All Act
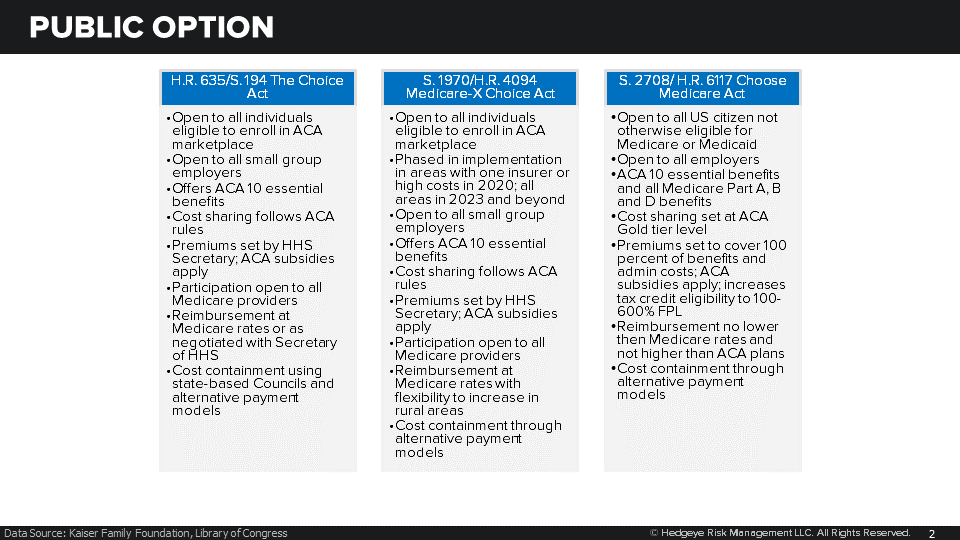
- H.R. 635/S. 194 The Choice Act
- S. 1970/H.R. 4094 Medicare-X Choice Act of 2017
- S. 2708/H.R. 6117 Choose Medicare Act
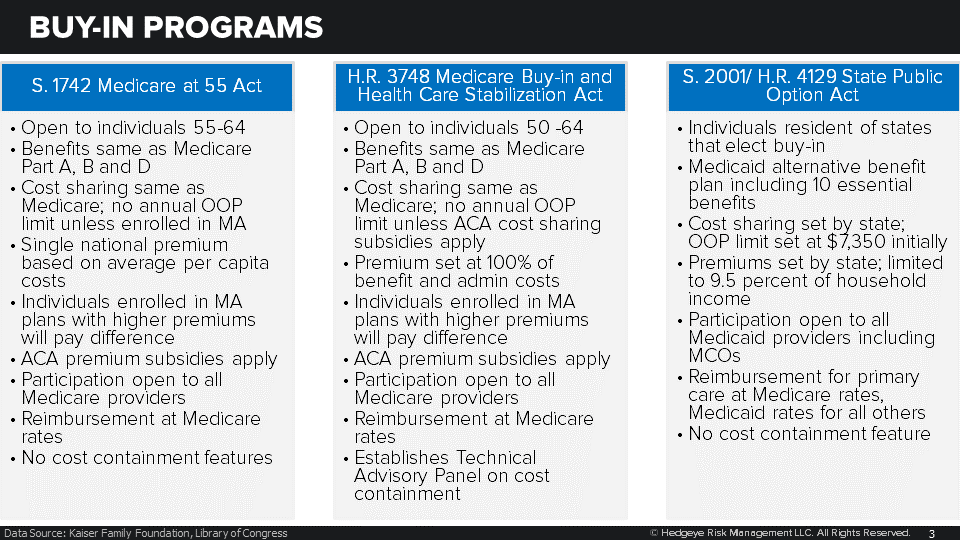
- S. 1742 Medicare at 55 Act
- H.R. 3748 Medicare Buy-in and Health Care Stabilization Act of 2017
- S. 2001/H.R. 4129 State Public Option
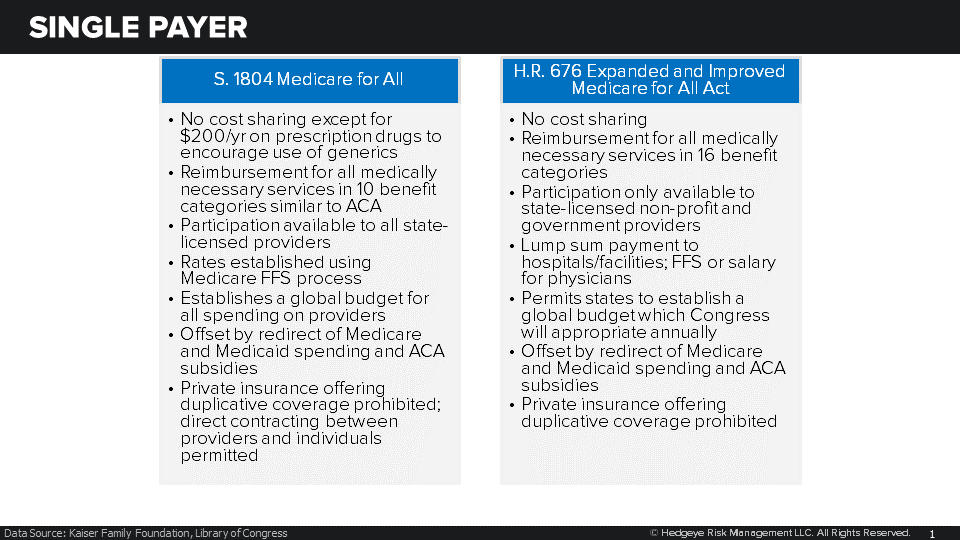
Medicare-for-All is, of course, the most disruptive and therefore least politically viable alternative, campaign speeches notwithstanding. In addition to effectively outlawing private insurance, these proposals would apply budgetary constraints to federal health insurance for the first time ever. Rates would have to be set within a global budget which is likely to have the effect of significant reduction in provider reimbursement.
With commercial subsidization of Medicare and Medicaid services eliminated, providers may elect not to participate in these programs and instead contract directly with individuals. Depending on market share of a health system, access issues could develop.
Single payer would, of course, be a major headwind for payers and many providers. Large, vertically integrated systems could develop the expertise to contract directly with individuals, thus mitigating some of the impacts. Other providers would have to accept significantly reduced rates.
A public option would permit a government-sponsored insurer to operate in competition with commercial insurers on the ACA exchanges. The public option was seriously considered and part of earlier drafts of the ACA, suggesting a higher level of viability than single payer. In areas of the U.S. with one or two ACA marketplace insurers, the public option presents another alternative.
However, the proposed Medicare-level reimbursement rates may pose problems for implementation as providers avoid inclusion in public option networks when possible. Since the public option will limit reimbursement to Medicare rates, the premiums are likely to be more competitive than many ACA commercial plans. If these public option plans become popular enough, it might be difficult for providers to avoid them altogether.
The public option represents a significant headwind for payers and providers, given the reduced reimbursement and commensurate premium prices.
Finally, the Medicare or Medicaid buy-in option would permit people not otherwise eligible for these programs to enroll. Like the public option, buy-in programs would be at the discretion of the individual enrollee, making the whole concept politically alluring.
Buy-in programs would be a net positive for payers like UNH with a significant presence in the Medicare Advantage market. For providers, it would represent a diminution of commercially insured population and a corresponding reduction in reimbursement.
In this Congress, House Speaker Nancy Pelosi has pledged to hold hearings on Medicare-for-All and presumably a public option and buy-in programs. None of these bills will go anywhere as the Senate remains firmly opposed, which is the point. The hearings will highlight Democrats commitment to expanded government-sponsored health benefits and support presidential campaign messaging with an eye toward enactment in 2021. Health care was a winning issue for Democrats in 2018 and they plan on doubling down from now until Nov. 2020.
In the meantime, expect a lot of headline risk as the political press covers the issue closely.
Emily Evans
Managing Director – Health Policy
Twitter
LinkedIn