
We have believed since CMS initially sent it up the flagpole in 2015, that a new payment system for home health was an inevitability. However, the HHGM proposal last year was doomed from the start. If for no other reason, CMS’s rushed and poorly vetted proposal was designed to be implemented in an unprecedented “partial budget-neutral” – whatever that is - or “non-budget neutral manner.” Hacking a few billion dollars out of a Medicare program was bound to attract Members of Congress – which it did.
The story is told around Washington that finalization of the HHGM was included in the CY 2018 final rule until shortly before its release. CMS staff eliminated the relevant text at the last minute and replaced it with a terse, scolding message to the industry. Our reading of the CY 2018 final rule was that Home Health operators had better get prepared for large-scale changes in how CMS pays them, the CY 2018 hiatus notwithstanding.
To address the more noxious provisions of the CY 2018 proposal, Congress intervened in February and required that the HHGM – now known as the Patient Driven Groupings Model – to be budget neutral, thus eliminating the industry’s most credible – and easily understood - objection.
Congress’s direction also calls for consideration of other payment models including those offered during the CY 2018 comment period. It required at least one Technical Expert Panel to convene between Jan. 1, 2018 and Dec. 31, 2018 to vet and discuss a new payment model. To make all these things happen, Congress directed CMS not to implement a new payment system until after Jan. 1, 2020.
The message from Congress was clear. CMS was to develop some consensus within the industry before making a new proposal. For that reason, our preview note in May suggested that CMS would provide loads of guidance and signals but not a formal proposal.
The bureaucracy was having none of that.
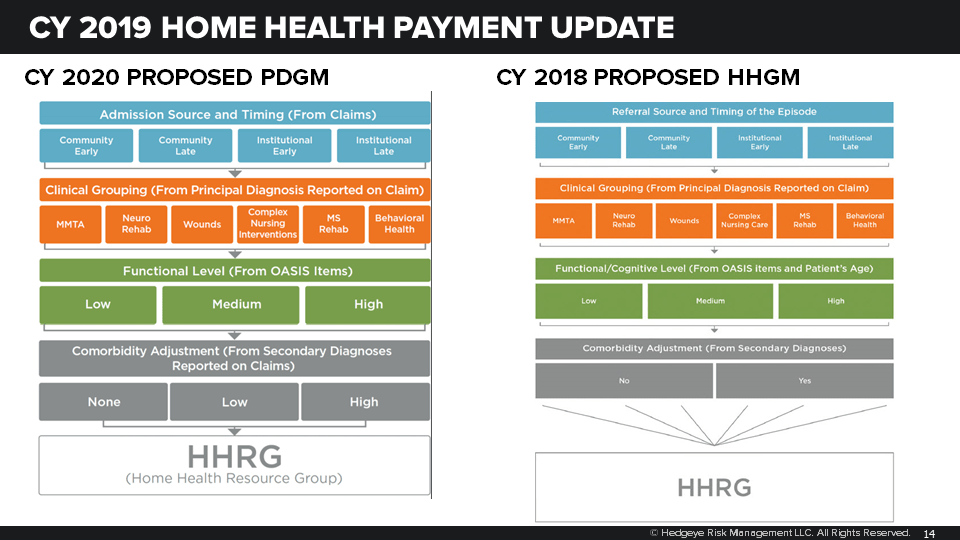
The CY 2019 proposed rule calls for implementation of a new payment system in CY 2020 that is very similar to the HHGM in the CY 2018 rule. The new Patient-Driven Grouping Model uses a very similar classification of patients by admission source, clinical group, function group and the presence of comorbidities. Despite concerns from the industry, the PDGM includes just one minor adjustment accounting for comorbidities.
The proposed amount does account for budget neutrality and resource use in a 30-day episode that should be more acceptable to the industry. Instead of allocating half the estimated CY 2019 standard episode payment, or about $1,500, to the new 30-day payment unit, CMS is proposing between $1,700 and $1,800, depending on certain behavioral assumptions.
For the life of use, we find scant evidence that CMS is interested in Congress’s other guidance. CMS asserts that a Feb. 2018 TEP that was convened before the budget deal passed met the requirements of the statute. They are correct when it comes to the letter of the law but certainly not its spirit. We also see little in the rule that suggests CMS gave consideration to other payment models – like that submitted by AFAM – offered during the CY 2018 comment period.
Expect the industry to howl – and some of it will be justified – but don’t expect CMS to relent much, if at all.
We will dive into this deeper next week after other Medicare rules have been released. To be sure, PDGM represents a significant change to the industry and it will need to adapt. The good news is that large, well-capitalized providers are better positioned to adjust and adapt.
Payment Update. The annual payment update is quite favorable, a reflection of the end of ACA and other legislative pay-fors. The standard episode payment will increase from $3,040 to $3,151. Overall, Medicare will spend 2.1 percent more on home health services in CY 2019.

The payment update is a reflection of the expiration (finally!) of ACA and other legislative pay-fors.
Rural Add-on. The February budget deal also extended the expiring rural add-on payment but with strings attached. The payment will now vary depending on where the home health agency is located. High utilization counties – defined as 17.72 episodes per 100 beneficiaries – of which there are 510, will receive a 1.5 percent payment adjustment in CY 2019. Low population counties – defined as six individuals or fewer per square mile – of which there are 334, will receive 4.0 percent in CY 2019. The remaining 1,162 counties will receive a 3.0 percent add-on payment.

Remote Patient Monitoring. The proposed rule continues CMS’s bias toward supporting telemedicine by permitting home health agencies to account for RPM as an administrative expense on their cost reports. RPM will still not be separately billable – which is what it will take to increase use above the 3 percent of agencies that currently offer RPM.
It is so hot the shade is looking for shade so we won’t be outside if you call with questions.
Emily Evans
Managing Director
Health Policy
Twitter
LinkedIn
