Tomorrow afternoon CMS will host an open door forum on Home Health, Hospice and Durable Medical Equipment. On the agenda is the possible switch from the Home Health PPS (HHPPS) reimbursement system to a Home Health Resource Group (HHRG) regimen. As we noted in our June 27 report, CMS had hinted at a new payment system in the FY 2016 annual update and then expanded on the idea in the FY 2017 rule. As we said in that June note, time is the most precious of commodities in government. If CMS is spending time on a new payment structure, you can be assured they mean to pursue its implementation.
With the announcement, CMS released a power point presentation from its Home Health payment contractor, Abt Associates. That presentation sheds a little more light on what they are considering.
Background. There are approximately 12,500 home health agencies in the U.S. serving about 3.5 million distinct beneficiaries. Home health patients must meet two major requirements to qualify for service; they must be home bound and they must require skilled care. Unlike other post-acute settings, home health stays need not be preceded by a hospital stay. Also, unlike other post-acute settings, home health beneficiaries are not required to make a copayment
Patients, when they are admitted to a home health agency, are assigned to a Home Health resource Group (HHRG). There are 153 HHRGs into which a patient is classified based on whether the episode is early (episodes one and two) or late (episodes three and higher); the patient’s clinical severity, functional status and level of resource needs. Table 1, illustrates a sample of HHRGs in use:
Table 1: Sample List of Home Health Resource Group Classifications
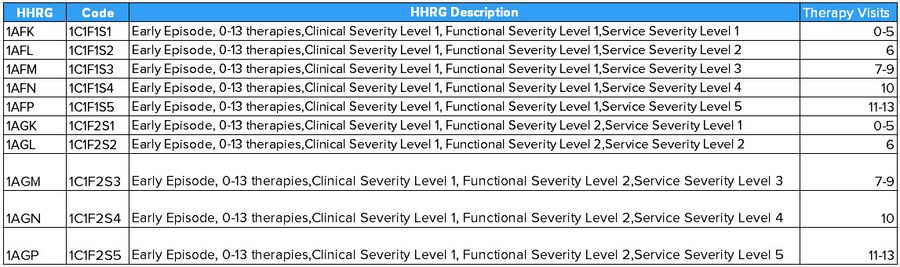
Source: CMS
It is the use of therapy as part of the classification system that has long been criticized by policy makers. Since at least 2011, the Medicare Payment Advisory Commission (MedPAC) has recommended a change in payment policy that eliminates therapy visits as a criteria for reimbursement.
Linking therapy visits to payment also runs counter to post-acute reform that has long been the holy grail of policy efforts. The IMPACT Act of 2014 requires a post-acute reform recommendation in 2020. Those reform efforts are focused on payment that is driven by patient characteristics instead of the somewhat arbitrary determinants of therapy visits and the type of building housing the patient.
The Affordable Care Act mandated a report on home health utilization and access to care, particularly for vulnerable populations. That report was delivered to Congress in 2014. The report goes on to say that CMS could implement changes that addressed the findings of the report via a demonstration provided they proposed one no later than Jan. 1, 2015. CMS did deliver the report – several months late. CMS did not propose a demonstration as stipulated by the ACA.
In the FY 2016 reimbursement update released last summer, CMS cited the ACA-mandated report as the basis for considering changes to the home health reimbursement system. They disclosed three possibilities for changes to the payment system. These were:
- Diagnosis on Top Model (DOT) – This payments system would combine diagnosis groups with a regression model to create separate weights for patients with different diagnosis. Under the DOT model, episodes would be first divided into different diagnosis groups, before determining the clinical and functional levels. Payment model regressions would be run separately for each diagnosis group.
- Predicted Therapy Model – This payment model option would be similar to the current payment model in that actual therapy visits used in the current HHPPS model would be replaced with predicted therapy visits to develop case-mix weights and payment amounts on the predicted number of visits. The case-mix weights would be constructed via a two-part model. The first part would use a logistic regression to estimate whether or not the episode had any therapy visits. The second part of this predicted therapy model would use binomial regression to estimate the amount of therapy visits conditional on having any therapy visits.
- Home Health Groupings Model -The premise of this model is that it starts with a clinical foundation and groups home health episodes by diagnosis and the expected types of home health interventions required. Using clinical judgement, each diagnosis code would be assigned to one of seven groups. Those seven groups include:
- Musculoskeletal Rehabilitation
- Neuro/Stroke Rehabilitations
- Skin/Nonsurgical Wound Care
- Post-Op Wound Aftercare
- Behavioral Health Care
- Complex Medical Care
- Medication management, Teaching and Assessment
The HHG Model would not include any therapy thresholds. It would take into consideration other items such as whether or not the patient was admitted from an acute or post-acute care settings. According to CMS, the HHG Model would group home health episodes in a way that mirrors how clinicians differentiate between different types of beneficiaries. After describing these possibilities for changes to the payment system, CMS indicated that they would be studying the issue more and would issue a technical report and provide other information in the future.
Throughout the rest of 2015 and early 2016, CMS provided little indication that they would move forward with a payment system change. Then, in the FY 2017 annual payment update proposed rule released in late June, CMS included a more detailed description of the HHG Model. While not offering any specific proposals, as we said in our June 27 note, CMS was clearly signaling plans to move forward with a change.
CMS’s expanded description of the HHG Model included the previously mentioned clinical groupings. Other payment considerations would be:
- Timing- Episode would be placed into just two groups “early” and “late.” Currently, the first two 60-day episodes are classified as “early” and the third and subsequent episodes are “late.” In the proposed rule, CMS disclosed recent analysis that showed there is a substantial difference in the number of visits that occur during the first 30 days of a 60-day episode of care compared to the second 30 days.
- Referral Source – Episode would be classified into one of three referral source categories: acute, post-acute and community. According to CMS, patients admitted to home health from the community, an acute care setting or a post-acute provider had different observable patterns of resource use and would, under the HHGM, be paid differently.
- Clinical Groups – Episode would be classified under a diagnosis group according to ICD-9 Codes. These groups are: Musculoskeletal Rehabilitation, Neuro/Stroke Rehabilitation; Wound Care; Medication Management, Teaching and Assessment; Behavioral Health Care; and Complex medical Care
- Functional/Cognitive Level – Episodes would be grouped based on high, medium and low functional/cognitive level.
- Comorbidities – Episodes would lastly be classified based on the presence of secondary diagnosis.
The result of this multitier classification system would be 324 case-mix groups into which an episode of care would fall.
The expressed purpose of the HHG Model would be to address the high degree of variability in Medicare margins that exist throughout the current HHPPS system.
CMS closed out this portion of the FY 2017 proposed payment update rule by indicating they would release a more detailed Technical Report in the future. They also indicated they would be releasing a list of ICD-9 and ICD-10 codes assigned to each of the clinical groups described above so the industry could provide feedback.
On Thursday evening, without much fanfare, CMS posted notice of an Home Health, Hospice and DME Open Door Forum and included in the agenda an update on changes to the Home Health payment system. They also, quite helpfully included a link to their consultant’s report that previews much of what will be discussed tomorrow.
HHG Model Under Consideration. The report released with the announcement of the Open Door forum represents the current thinking by CMS but is not a concrete proposal. Based on what has been released, CMS appears to be considering a classification system that results in 128 different payment groups, and is thus a more simplified version of what they were pondering in late June. Episodes would be classified using five considerations:
- Timing; Early or Late
- Referral Source: Community or Institutional
- Clinical Grouping: Musculoskeletal Rehabilitation; Neuro/Stroke Rehabilitation; Wounds; Medical Management Teaching and Assessment; Behavioral Health or Complex Nursing Care
- Function/Cognitive Level: For Musculoskeletal Rehabilitation and Behavioral Health episode would be classified as low or high. For other clinical groups, patient would be classified as low, medium and high
- Comorbidity Adjustment: Yes or No depending on presence of secondary diagnosis.
Graphically, the classification system, of adopted, would look like this:

Source: CMS and Abt Associates
Another big change to the Home Health payment system would be that episodes would have duration of 30 days instead of the current 60-days. CMS’s research indicates that most visits occur within 30 days of admission. The first 30-day episode would be classified as early and all subsequent episodes would be classified as late. As is the case today, there would be no limit on the number of episodes.
Possible Impacts. The purpose of the change under consideration is to discourage unnecessary therapy utilization and encouraged skilled nursing care especially for patients that:
- Needed parenteral nutrition
- Were admitted with traumatic wounds or ulcers
- Required substantial assistance in bathing
- Were admitted following an acute or post-acute stay
- Had high HCC scores
- Had poorly controlled clinical conditions
- Were dual eligible
These motivations would suggest that Home Health Agencies whose episodes were more concentrated in those HHRGs with a high number of therapy visits would be negatively impacted by the change. LHC Group has long asserted that they were less dependent on therapy care than other agencies and the data appears to bear that out.
Table 2 below shows a breakdown of home health episodes by the major therapy categories for the largest publicly traded home health companies. Included is one private regional firm, Bayada as a point of reference. Please note that this table is derived from 2013 utilization data. In 2013, the ACA-mandated rebasing had not yet been implemented. For that reason, agency reaction to that payment change is not accounted for by these data.
Table 2: Home Health Episodes by Provider and Therapy Utilization.
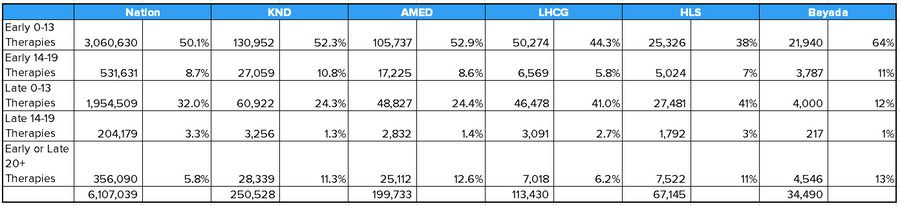
Source: CMS and Hedgeye
Another purpose for the change in the payment system is to reduce the level and variability of Medicare margins. As CMS and MedPAC have noted repeatedly, a case-mix system that properly accounts for resource use will exhibit uniform margins at levels CMS finds acceptable (i.e., not over 10 percent). According to the ACA-mandated report that looked at 2010 cost and payment data, all but two of the 153 HHRG had margins below 10 percent. Fifty-four of the HHRGs has margins in excess of 25 percent. (Note: Medicare margins are not financial margins. Medicare margins simply express the difference between the Medicare payments and the approved Medicare costs associated with that care.)
Table 3 below shows the distribution of home health episodes by HHRG that were reported to have margins that exceed 30 percent. Please note, these margin data are derived from 2010 cost and payment reports and do not account for case-mix adjustment in 2011 or rebasing in 2014, both of which may have affected admission and patient classification patterns. The episode data are derived from 2013 utilization reports.
Table 3; Home Health Episodes by Provider and High Margin Home Health Resource Group
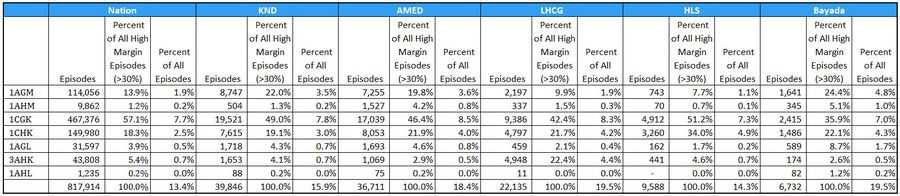
Source CMS and Hedgeye
Of concern is the inclusion of a referral source in the new payment system under consideration. CMS and MedPAC have both noted that increasingly home health patients are admitted from the community instead of an institutional setting like a Skilled Nursing Facility or an Acute Care hospital. The report to be discussed tomorrow includes a finding that about 2/3 of home health episodes are accounted for by community referral. Both CMS and MedPAC assert that the resources needed to treat a patient admitted to home health from the community are less than those needed to treat a patient admitted from an acute or post-acute institution.
Alleviating our concern about the referral source and the stated objective to reduce and make margins uniform, is our belief that what CMS proposes will likely be budget neutral. Assuming that is the case, the new payment system should shift reimbursement from patients who need therapy like those recovering from major joint replacement to those that need more skilled nursing care for other post-surgical recoveries. The addition of behavioral health provides an interesting addition with possibilities we had not considered until recently.
We are also concerned that the payment system under consideration is a pretty significant change and includes a more nuanced approach. CMS has struggled with communicating to its Medicare Administraive Contractors and getting them to follow instructions on changes just like this one.
Finally, it is unclear how frequently CMS will require recertification under a 30-day episode system. Recertification and the physican's face-to-face requirement have been a barrier for many providers who struggle with physician cooperation.
On the plus side, this new payment system looks to use like one that will encourage more comprehensive nursing care in the home - the most desired place for most people to recieve care.
Details on the call:
Conference call is at 2:00 EDST tomorrow. To participate by phone: Dial: & Reference Conference ID: 42968600
Encore available two hours after call ends. Instructions for recording: Encore: ; Conference ID: 42968600
Call with questions.