
With no forecast error adjustment, a declining multifactor productivity adjustment and an improving market basket index, SNFs are expected to see an additional $920 million in spending in FY 2017 compared to an estimated increase of $430 million in FY 2016 or 2.4 percent.
The rate increase reflects a market basket increase of 2.7 percent less a multifactor productivity adjustment of 0.3 percent. The difference between the forecast FY 2015 market basket and the actual FY 2015 market basket (the most recent year for which there is historical data) is 0.2 percent. Because the difference is less than 0.5 percent the forecast error adjustment is not triggered. Table 1 lists the rural and urban per diem payments for SNF providers for FY 2017.
Table 1: FY 2017 Per Diem Rates for Skilled Nursing Facilities

Source: CMS
The big news in the final payment update is the start of the SNF Value-based Purchasing Program which was imposed by the Protecting Access to Medicare Act of 2014. PAMA required just two things for the SNFVBP program – an all-cause, all condition hospital readmission measure which is to be replaced as soon as practical by an all-condition risk-adjusted potentially preventable hospital readmission measure AND private and public reporting. Beginning in October 2018, Medicare will begin adjusting payments to SNFs based on performance on these measures.
The first of these quality measures, the 30-day All-Cause Readmission Measure (NQF#2510) was adopted in the FY 2016 final rule. The “SNF Readmission Measure” (SNFRM) assesses the risk-standardized rate for all-cause, all condition, and unplanned inpatient hospital readmissions of Medicare fee-for-service SNF patients within 30 days of discharge from an inpatient hospital.
For the second of these measures CMS proposed to use the SNF 30 day Potentially Preventable Readmission Measure (SNFPPR) as the SNF all-condition risk-adjusted potentially preventable hospital readmission measure to meet the requirements of PAMA. This proposed measure assesses the facility –level risk standardized rate of unplanned, potentially preventable hospital readmissions for SNF patients within 30 days of discharge from an inpatient hospital.
Unlike the SNFRM, the SNFPPR is a quality measure that was not developed under the auspices of the National Quality Forum. Instead, it has been developed internally by CMS. The measure is also unique in that it measures readmission within 30 days of the hospital discharge instead of within 30 days of discharge from the Post Acute Care setting as is the case with the IRF measure.
For patients readmitted to the hospital while still at a SNF, the Potentially Preventable Readmissions (PPR) will be categorized into four clinical groups:
- Inadequate management of chronic conditions
- Inadequate management of infections
- Inadequate management of other unplanned events
- Inadequate injury prevention
For patients that are readmitted after leaving the SNF, the PPR conditions will be categorized into three clinical groups:
- Inadequate management of chronic conditions
- Inadequate management of infections
- Inadequate management of other unplanned events
The SNFPPR measure will be calculated for each individual SNF based on the ratio of the predicted number of risk-adjusted, unplanned, potentially preventable hospital readmissions that occurred within 30 days of discharge from the prior proximal hospitalization, including the estimated facility effect to the estimated predicted number of risk-adjusted, unplanned, hospital readmission for the same individuals receiving care at the average SNF. A ratio above 1.0 indicates a higher than expected readmission rate while a ratio below 1.0 indicates a lower than expected readmission rate. The readmission ratio is referred to as the Standardization Risk Ratio (SRR). The SRR is then multiplied by the overall national raw rate of PPR for all SNF stays. The resulting rate is the risk-standardized readmission rate (RSRR) of potentially preventable readmissions.
SNFs will be evaluated in two ways; on an improvement standard and an achievement standard. The achievement standard will be the 25th percentile of national SNF performance on the quality measure during a baseline period of Jan. 1, 2015 to Dec. 31, 2015. Achievement will be measured against a benchmark of the mean of the top decile of SNF’s performance on the quality measure. The benchmark, according to CMS, will reflect observed scores for the group of the highest performing SNFs. SNFs would receive points along an achievement range, which is the scale between the achievement standard (or threshold) and the benchmark during the performance period.
SNFs will also be evaluated on an improvement standard. The improvement standard (also known as the improvement threshold) is the individual SNF’s performance on the quality measure during the baseline period. During each performance period, CMS will compare the improvement score to the baseline to measure improvement.
The numerical values of the achievement threshold and the benchmark will be published in the final SNF payment rule and in any event not later than 60 days before the beginning of the performance period. The numerical values for the achievement threshold and the benchmark for FY 2017 are listed in Table 2 below:
Table 2: FY 2017 Numerical Values for Achievement Threshold and Benchmark
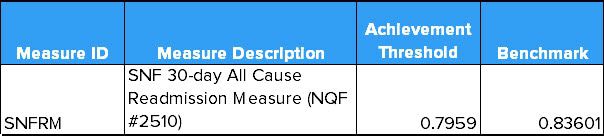
Source: CMS
Each SNF will be scored on a scale of 0 to 100 for achievement and 0 to 90 point scale for improvement. The scoring system calls for inverting the SNFRM rates so as to not confuse the public which may not associate a low rate with a positive result. A SNFRM of 0.15 would then be inverted to 0.85.
To calculate the achievement score, CMS will assign a score of 100 (the maximum) for any SNF that exceeds the benchmark. For any SNF whose score falls below the threshold, the SNF would receive a score of 0. For everyone in between, the achievement score would be calculated using this formula:

Source: CMS
To calculate the improvement score, CMS would assign a score of 0 to 90 based on how much a SNF’s performance on the quality measure improved from its performance on the measure during the baseline period. Each SNF would be assigned an improvement range that defines the distance between the SNF’s baseline period score and a national benchmark. The national benchmark would be defined as the top decile of SNF performance on the measure during the baseline period.
If a SNFs improvement score was equal to or lower than its improvement threshold, the SNF would receive a score of 0. If the SNFs performance period score was equal to or higher than the national benchmark, it would receive a score of 90. For all other SNFs the improvement score would be calculated using the following formula:

Source: CMS
In the final rule, CMs provides a few examples applying the scoring method. The example below is probably best illustrative of a real world example as most SNF’s will be scored within the achievement of improvement range.
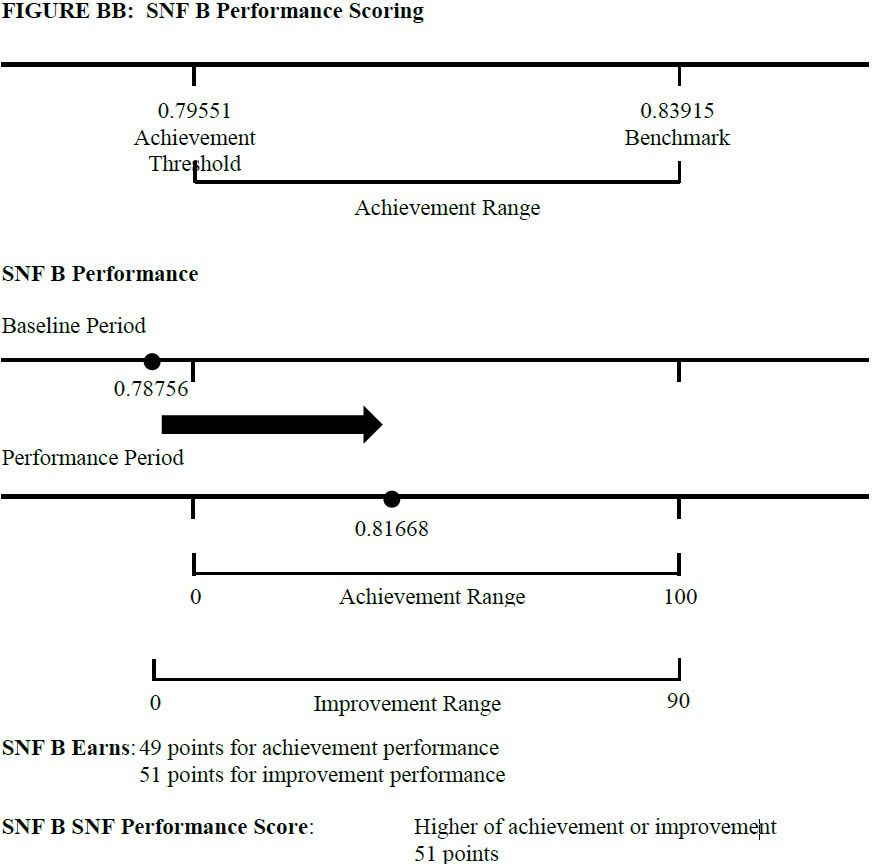
Source: CMS
CMS will use the higher of the achievement and improvement score to calculate incentive payments under the SNFVBP. The SNFVBP is NOT budget neutral. The total amount of value-based incentive payments must be greater than or equal to 50 percent, but not greater than 70 percent, of the total amount of reductions to payments for that particular fiscal year. The lowest 40 percent of SNFs must receive a payment that is lower than that they would otherwise be paid under the SNFPPS.
CMS will post performance scores and ranking on the Nursing Home Compare website and such other information as determines appropriate in future rulemaking.
Although only 95 comment letters were submitted to CMS for this final rule, most focused on the VBP program. Given the content of those comments, there appears to be some trepidation on the part of SNF providers. Also, given the decentralization of the sector, we suspect that many providers are not up to speed as they should be. However, at least initially, we do not believe the SNFVBP will be that much of a negative. CMS has selected as an achievement standard the 25th percentile of all SNFs – which is a much lower bar than the 50th percentile selected for hospitals. As is becoming common whenever the subject of value-based and alternative payment models comes up, responses to the SNFVBP provisions were concerned about adjustments for socio-economic factors. CMS struggles with this argument because at this point there is no real agreement on how to adjust for socio-economic factors without perpetuating the status quo of low quality care.
The SNFVBP represents the same challenge for providers that the Home Health Value-based Purchasing Program does. It provides, for really the first time, Medicare's expectations about the care they pay for in skilled nursing facilities. Unlike other VBP programs the SNFVBP will rely on just one quality measure - hospital readmissions. This constraint specified by law will likely limit nuance in the program but will keep providers focused on the thing that has plagued the care setting for years. The SNFVBP also addresses a long standing gripe of hospitals who are also evaluated on readmissions. Patients sent to SNFs often return to the hospital because of poor care at the SNF not at the hospital. The alignment of interests between these two care settings should be a positive for the hospital sector and lead to better care coordination between the two setting.
