|
Editor's Note: Below is a brief excerpt from a complimentary Health Policy Unplugged note written by our Health Policy analyst Emily Evans. Click HERE to learn more about Emily's research process and the analysis subscribers receive. |

Politics
For the last 20 years, it seems anyone in Congress who gets regular attention from those media organizations that make their way to the kitchen tables of well-educated, generally prosperous urban Americans are obsessed with “going big,” when just solving the problem in front of them would suffice.
President Barack Obama could have had a popular health care bill that supported the purchase of individual insurance by offering similar preferential tax treatment employer-sponsored insurance enjoyed.
Instead, he “felt lucky” and pushed for a wide -ranging mess of a bill whose contradictions and inconsistencies have been the preoccupation of courts ever since.
Other than some of the Medicaid provisions – a program that could hardly be called a contributor to good health – the ACA failed to live up to both its potential and its promise.
The latest effort to go big is the reconciliation bill known as Build Back Better. Speaker Pelosi has called it “the culmination of my career in Congress.” White House Spokesperson, Jen Psaki at a recent briefing said, “The President wants to make fundamental change to our economy and feels coming out of the pandemic is exactly the time to do that….and we’re not going to have the same opportunity to do it for some time.”
Going big, in other words, is the necessary response to the inexorable march of time. Implicit in that urgency is a recognition that the policies in the Build Back Better bill are not responses to actual problems but a wish list of programs that fulfil personal or political aspirations. As a result, many of those goals are disconnected from and may make the problems at hand much worse.
The most critical problems for health care are on the supply side. Labor is stretched thin, inputs for things like pharmaceuticals, supplies, fuel and devices are rising.
While the policy fig leaf of inflation as transitory works to explain absent response to supply prices, there is no getting around the magnitude or the durability of labor shortages in health care.
Most of Build Back Better is focused on the demand side. More or more rich insurance coverage is the primary objective. Also included is a stunningly large obligation to Medicaid Home and Community Services program that provides home care to the elderly poor and disabled.
Even if the definition of home care worker is extended to include one’s family member, as expected, one still wonders where the workers will come from to provide the level of service contemplated by the bill.
Policy
The BBB is not entirely without a response to labor problems. It includes about $150M for nurse placement in maternal and perinatal clinical settings.
There is also money to expand nurse training and consideration is being given to a policy that mandates staffing ratios at nursing facilities. Notwithstanding the hit AMN took last week, all policies related to nurse staffing are a positive for the staffing business.
These responses, while important, may not start to move the needle on supply for several years. Meanwhile demand for services due to filling the Medicaid gap, extending ACA subsidies, and expanding the scope of benefits for Medicare are slated to go into effect, at least in part, in 2022.
There is a good chance some of that will get delayed. Filling the Medicaid gap has potential for a painful execution, for example.
Also relevant, provisions to address labor shortages were not in early drafts of the Build Back Better framework. It took the Federation of American Hospitals’ involvement to get the White House to consider the current field conditions.
As Members of Congress make their way back to The Hill, this week we will get some clarity on the prospects for the health care provisions and perhaps the bill in general. Time is not your friend when trying to get a bill of this magnitude passed. The more that goes by the likely its chance of failure.
Power
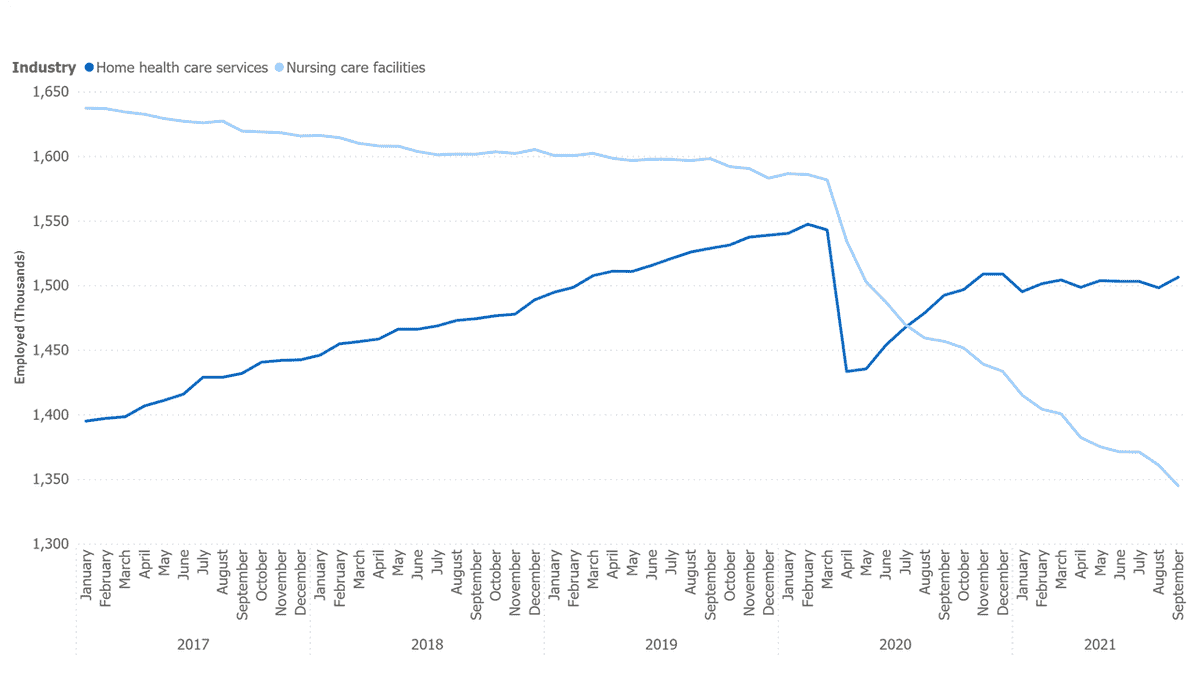
States are swimming in money after the American Rescue Plan’s passage in early 2020. It is no surprise that they have not needed to reckon with one of the most startling secular changes in health care, the demise of the nursing home industry.
There are two primary sources of revenue for state Medicaid programs: general fund and provider taxes. Provider taxes or fees generate revenue from specified categories of providers.
In most states, it is used as a mechanism to generate new in-state funds and match them with federal funds so that the state gets additional federal Medicaid dollars. In most cases, the cost of the tax is paid back to providers through an increase in the Medicaid reimbursement rate.
The two largest contributors of provider taxes are nursing homes and hospitals. Generally, the tax is assessed on licensed beds on a per diem basis. As people avoid nursing facilities either because of the reputational damage done by COVID, the absence of proper staffing or the more readily available and safer home care, the number of licensed beds will fall and, with it, tax collections to support the Medicaid program.
The rebalancing of revenue needs, once the tide of cash recedes, will be one symptom of the COVID relief hangover. Given the red tinge of most states, expect legislatures to use it as a way to rein in the program, one way or another. (MOH, CNC, ANTM)
My head hurts already.